Stroke EVT- A Discussion
•Download as PPTX, PDF•
8 likes•2,240 views

A sixty five year old female presented at five hours after symptom onset with a NIHSS score of 22. Imaging showed a right middle cerebral artery occlusion. The patient underwent mechanical thrombectomy using a stent retriever. Follow up imaging showed reperfusion of the previously occluded vessel and the patient was discharged with mild residual aphasia and a modified Rankin score of 2. Factors such as rapid triage protocols, minimizing delays from imaging to treatment, and standardized approaches can help reduce time to recanalization and improve outcomes in acute ischemic stroke.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (17)
Similar to Stroke EVT- A Discussion
Similar to Stroke EVT- A Discussion (20)
More from Dr Vipul Gupta
More from Dr Vipul Gupta (20)
Recently uploaded
Recently uploaded (20)
Stroke EVT- A Discussion
- 2. 26 female wake up stroke; NIHSS 22; R sided weakness and aphasia
- 3. Solitaire (ev3)- 2012, Trevo (Stryker), Revive™ SE (Codman), Etc…. etc….. Stentretrievers - Stent or stent-like system for clot removal
- 4. ARTS (SOLUMBRA) (Aspiration-Retriever Technique for Stroke)
- 5. Techniques.. ADAPT… A Direct Aspiration First Pass technique
- 6. Techniques A. Stent retriever B. Stent retriever with BCG C. Stent retriever with DAC (ARTS), SOLUMBRA D. ADAPT E. Other
- 7. Issues • Trials • Simplicity • Change of techniques • Cost issues • One standard technique
- 8. P to P – 58 minutes Puncture to reperfusion – 18 minutes
- 9. F/U MRI; Some residual mild aphasia
- 10. Technique • Simple – similar result in different hands and at all times • Fast – stick to one technique • Each step as a protocol – everybody in team in sync • Avoid experimentation in initial phase • Other factors (selection, time …) more important
- 11. Device – technique Comparison of protocol- Randomised (Intervention Vs Standard medical therapy)
- 12. TREVO, Stryker Neurovascular REVIVE, Codman Neurovascular ERIC, Microvention Technique ……
- 13. Choice of Stent retriever and why ? A. Solitaire B. Trevo C. Revive D. ERIC E. Other
- 14. 14 Presentation Title (Edit on Slide Master) | June 1, 2015 | Confidential, for Internal Use Only SOLITAIRE 2 - IMPROVED TENSILE STRENGTH Solitaire™ 2 Device Solitaire™ FR Device The Solitaire™ 2 Revascularization Device also employs a redesigned attachment zone offering a 2x improvement in joint strength designed to eliminate unintended detachments 0 2 4 6 8 10 12 14 Peak Load Solitaire™ FR Device Solitaire™ 2 Device ( N )
- 15. 15 Presentation Title (Edit on Slide Master) | June 1, 2015 | Confidential, for Internal Use Only SOLITAIRE 2 Device overview Reference Number Recommended Vessel Diameter (mm) (A) Total Length (mm) (B) Retrieval Zone (mm) (C) Device Diameter (mm) (D) Push Wire Length (cm) (E) Distal Markers (F) Proximal Markers Distance from Distal Tip to Flourosafe Marker (cm) Micro Catheter ID (in) SFR2-4-15 2.0 - 4.0 26 15 4 180 3 1 <130 .021 SFR2-4-20 2.0 - 4.0 31 20 4 180 3 1 <130 .021 SFR2-4-40 2.0 - 4.0 50 40 4 180 3 1 <130 .021 SFR2-6-20 3.0 - 5.5 31 20 6 180 4 1 <130 .027 SFR2-6-30 3.0 - 5.5 42 30 6 180 4 1 <130 .027
- 16. Trevo and Trevo XP High Integration Radial Force Large Cell Size with Low Coverage Tubular Design INTEGRATE & PULL Photograph taken by Stryker Neurovascular.
- 17. Solitaire™ FR Device vs. Trevo™* Device Design Overview **Competitive Testing Report FD2815. ***Covidien Testing Data: FD2601A Trevo™* Device Solitaire™ DeviceImages property of Covidien. Image is an artistic rendering and not a n exact depiction of the Solitaire™ FR Device. Image property of Covidien. Image is an artistic rendering and not a n exact depiction of the Trevo™ Device. • The Solitaire™ FR device - Parametric™ design that may provide multiple planes of clot contact. •Trevo - straight cut tube ; struts of the Trevo™* device to cut into the clot Consistent Cell Size Variable Cell Size Force- Flex™ Straight- Cut
- 18. 64 year old man with left hemiparesis, bought to emergency in 60 min, NIHSS 1 No improvement after IV tpa 54, M, 2 hours, NIHSS - 17
- 19. Tandem – Proximal ICA occlusion (AS) with MCA clot A. Distal followed by proximal PTA/Stent B. Proximal PTA followed by distal C. Proximal stent followed by distal D. Proximal suction followed by distal E. Distal with no proximal intervention
- 22. Follow up Patient Improved mRs 2 at discharge CTA 15 days later show occluded stent Right MCA opacifies through Acom
- 23. Anterograde vs retrograde approach: Antegrade : Stenting first Pros: Access to distal lesion Perfusion through collateral (in case of tandem MCA occlusion) Reduced risk of repeat embolism (??) Cons: Delay in reperfusion of occluded territory Retrograde: Thrombectomy first Pros: Early reperfusion of occluded territory Cons: Access to distal lesion is limited Risk of repeat embolism (??)
- 24. Our approach Acute stroke with ICA occlusion • Usually distal first , take the guiding catheter across the stenosis • Terumo/microcatheter to cross • DAC/Neuron 6F - aspiration • Co-axial approach • Recanalize the I/C part • Check the proximal ICA (wire in situ) • If good flow , not a severe stenosis - wait • Usually needs Angioplasty/stenting • Drugs – If IV tPA given – Ecospirin 150 mg, Clopidogrel 225 mg ; other wise 300, 450 mg
- 25. • 28 patients • Antegrade approach (85.7%); Reverse approach (14.3%) • Antiplatelet: Load Aspirin (650 mg) when stenting anticipated. • Cone-beam CT after tt - No hmg, 600 mg loading dose of clopidogrel. SICH in 2 (one received IV tPA)
- 26. • Retrospective; September 2010 and April 2013 • Compared proximal vs distal approach • Weight-adapted bolus of tirofiban followed by a continuous infusion for 24 h to prevent in-stent thrombosis • After exclusion of cerebral hemorrhage on follow-up imaging, 500 mg of acetylsalicylacid (ASA) and 300 mg of clopidogrel
- 28. Issues with Stenting in the acute setting: Factors to be considered. • Infarct core volume • Time to reperfusion • Received IV tPA or not • Antiplatelet to be tailored to above • Need for Abciximab in case of in-stent thrombosis (increases bleeding risk) • Risk of stent occlusion • Antiplatelet protocol: Thrombolysis (Yes) – Ecosprin (300); CT Brain in 12 to 24 hours no hemorrhage add Clopidogrel. • Thrombolysis (no) – Ecosprin 300 and Clopidogrel 600 loading
- 29. Emergency carotid stent – drug protocol A. Loading with abciximab or equivalent B. Loading with aspirin and clopidogrel C. CT followed by loading D. Single anti-platelet followed by second after a while E. Other
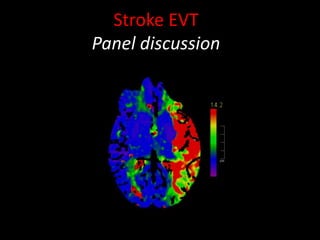
- 30. • 60 years old female. • h/o hypertension and hypothyroidism • Acute onset left hemiparesis and left facial weakness • No history of LOC/seizures • CT Brain , perfusion and angio done 6 1/2 hours after ictus.
- 33. 2 months later
- 34. A D A C B A E F HG A sixty five year old presented at five hours of symptom onset with a NIHSS of 22
- 40. Patient presented with in 2 hours Futile IV tpa 62/F, 3-hours, NIHSS 18
- 41. Imaging A. CT, CTA B. CT, CTA, collateral scoring C. CT, CTA, CTP D. MR – DWI, MRA E. MR – DWI, MRP, MRA F. CT, CTA, MR- DWI
- 42. Patient presented with in 2 hours Futile IV tpa
- 43. 26 female wake up stroke; NIHSS 22; R sided weakness and aphasia
- 44. Good collaterals by the Miteff method (OR, 3.341; 95% CI, 1.203–5.099; P .014) was the independent predictor of good outcome amongst various collateral grading scales. Arterial Collateral status – penumbra, retention of penumbra
- 45. Miteff system A, Contrast opacification all sylvian branches. B, Some vessels can be seen at the Sylvian fissure. C, distal cortical filling alone
- 46. Modified Tan system. A, Less than 50% of the MCA territory. B, More than 50% of the MCA territory
- 47. Multiphase CTA Better able to predict outcomes than single phase and perfusion CT
- 50. CT, CTA, CTP…. CT perfusion imaging MTTCBF CBV Quantitative CTP mismatch classification using relCBF and Tmax is similar to perfusion-diffusion MRI. Stroke. 2012 Oct;43(10):2648-53. Epub 2012 Aug 2. Incremental improvement in interobserver reliability was demonstrated for NCCT, CTA-SI, and CTP-CBV, respectively. (Stroke. 2013;44(1):234-6) 25.
- 51. CT perfusion • J Neurol Neurosurg Psychiatry. 2013 Jan 25. CT perfusion improves diagnostic accuracy and confidence in acute ischaemic stroke. CTP was more frequently diagnostic than NCCT (80% vs 50%, p<0.001). Normal CTP in 86/87 patients with stroke mimics supported withholding tPA Consideration of multiple available CT sequences increases confidence for correct stroke diagnosis among inexperienced readers and may facilitate identification of stroke mimics Stroke. 2013 Feb 12. [Epub ahead of print] Computed Tomography Workup of Patients Suspected of Acute Ischemic Stroke: Perfusion Computed Tomography Adds Value Compared With Clinical Evaluation, Noncontrast Computed Tomography, and Computed Tomography Angiogram in Terms of Predicting Outcome. Zhu G, Michel P, Aghaebrahim A, Patrie JT, Xin W, Eskandari A, Zhang W, Wintermark M. J Neurointerv Surg. 2012 Nov 26. [Epub ahead of print] CT perfusion-guided patient selection for endovascular recanalization in acute ischemic stroke: a multicenter study
- 53. •The Interventional Management of Stroke pilot trials tested combined IV/IA therapy onset. •Among the 54 cases, only time to angiographic reperfusion and age independently predicted good clinical outcome after angiographic reperfusion.
- 54. 30-min delay in angiographic reperfusion reduced the relative likelihood of a good clinical outcome by 12% i adjusted analysis.
- 55. What did ESCAPE trial aim for? P2P- picture to puncture P2R – picture to recanalization A. P2P - 90 min, P2R - 120 min B. P2P - 60 min, P2R – 120 min C. P2P - 60 min, P2R – 90 min D. P2P – 45 min, P2R – 60 min E. P2P – 30 min, P2R – 60 min
- 57. TIME for recanalization • Onset to door time • Door to Imaging/picture • Picture to puncture (P2P) • Puncture to recanalization time Hospital processes Technical skills • Onset to puncture/groin time • Onset to recanalization time • Door to Puncture (D2P) • Picture to recanalization (P2R) Society infrastructure Ultimate predictor
- 59. One hundred forty-six patients (93 pre- vs. 51 post-QI) were analyzed.
- 60. The worst clinical outcomes were noted with door-to-puncture times of 136 minutes or greater ( J Am Heart Assoc. 2014;3:e000859 N=478
- 61. P2P Challenges • CT vs MRI • Availability of the angiosuite SOS • 24x 7 neurointerventionist, anaesthetist, technician, nurse • Team of like minded people • Overcoming the Financial Barrier
- 62. Rapid Triage Protocol and Stroke Team Notification Single Call Activation System Changes at Medanta
- 63. Door time recording by CCTV footage Transfer Directly to CT Rapid Acquisition and Interpretation of Brain Imaging Multimodal imaging protocol (CTA/CTP) Parallel approach Clinical assessment ‘en route’ to Imaging. Access line and blood investigations (POC) Prepare IV tPA Alert Angio suite/ Lab personnel Financial considerations/ undertaking Consent – pre written Changes at Medanta
- 64. Puncture to Recanlization time • Planning on CT angiography • Local anaesthesia • No groin preparation • Putting Foley’s after deploying stent • Standardized stroke kit that is ready to go (Stroke. 2014;45:e252-e256.)
- 65. Tips to getting the clot on first pass • Use of balloon guide catheter • Long stent 4mm X 40 mm solitaire • Push & Fluff technique • Prayer!!!
- 66. • 41 year old male, Severe MR, EF 20% • Stroke in sleep, NIHSS 14 on admission
- 67. 6:22AM
- 68. Patient made gradual recovery Left LL 4/5 and UL 3/5 - 30 day follow up mRS at 90 days- 0
- 69. For more information on: STROKE & NEUROVASCULAR INTERVENTIONS: URL: www.sanif.co.in Facebook: https://www.facebook.com/strokeawarenessindia https://www.facebook.com/vipul.gupta.35175 Twitter https://twitter.com/drvipulgupta25 LinkedIN https://in.linkedin.com/pub/dr-vipul-gupta/51/8a1/25a YouTube Channel: Stroke & Neurovascular Interventions www.youtube.com/c/StrokeNeurovascularInterventionsfoundation Dr Vipul Gupta
- 70. Thank You