Downloaded 35 times
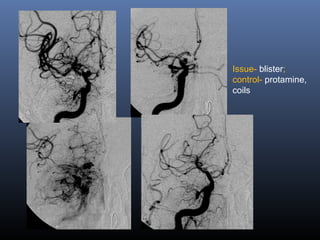
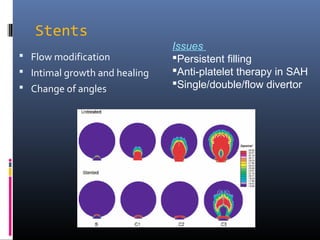
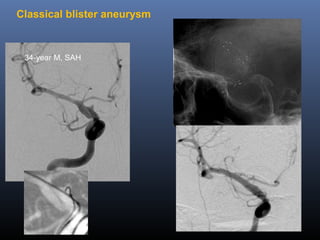
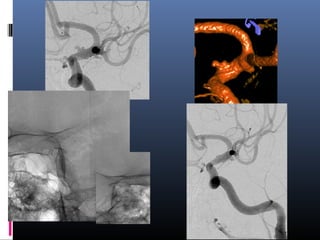
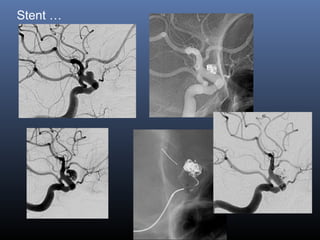
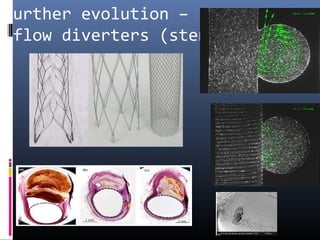

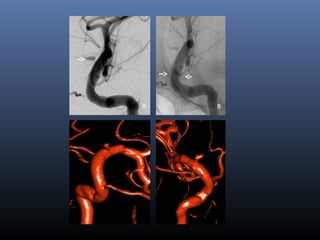
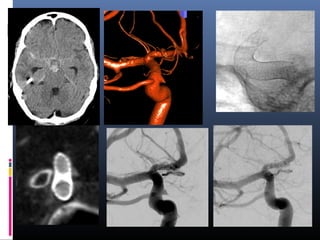
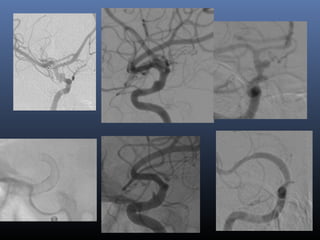
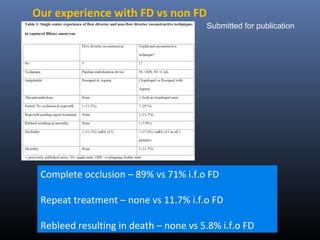
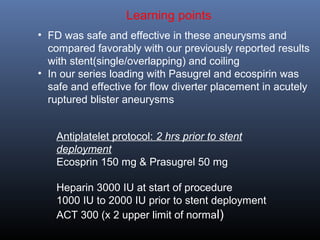
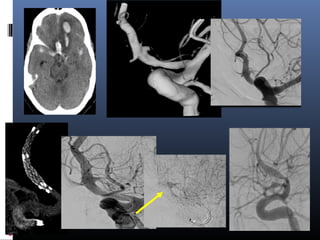

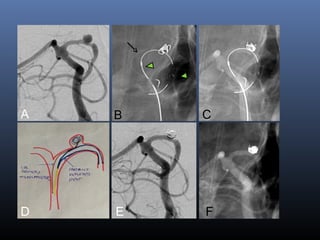
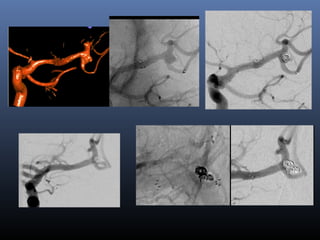
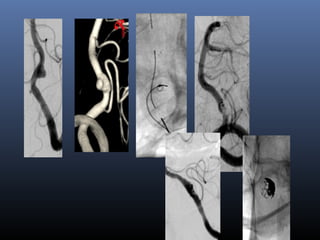
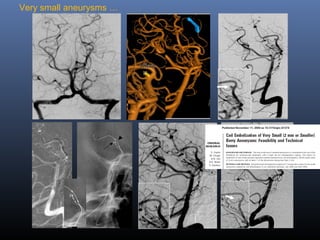

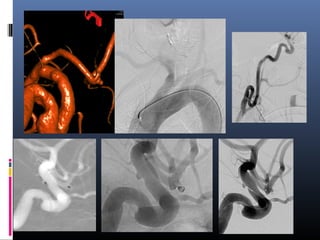


This document discusses blister aneurysms, which are rare lesions characterized by a hemispherical shape and fragile walls located in non-branching sites of arteries like the internal carotid artery. It notes that blister aneurysms are very small and atypical in location, making them difficult to treat surgically or with endovascular coiling. The document presents the author's experience using flow diverters like the Enterprise stent to treat 17 patients with blister aneurysms, finding a high rate of complete occlusion and no rebleeding or need for retreatment compared to other methods. It emphasizes the importance of detecting and recognizing small blister/dissecting aneurysms and having a careful antiplatelet protocol when using flow diverters in their


















































































