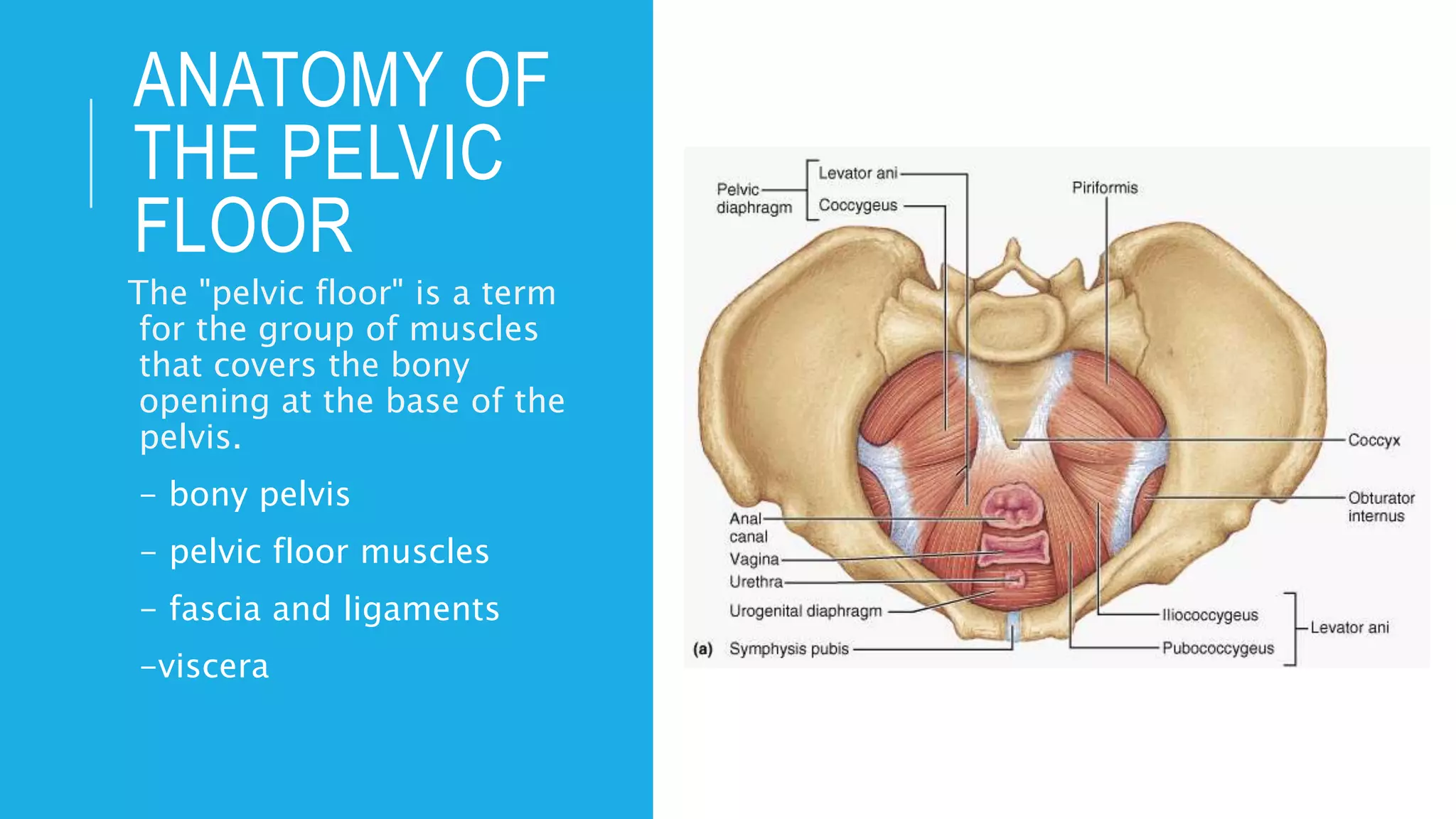
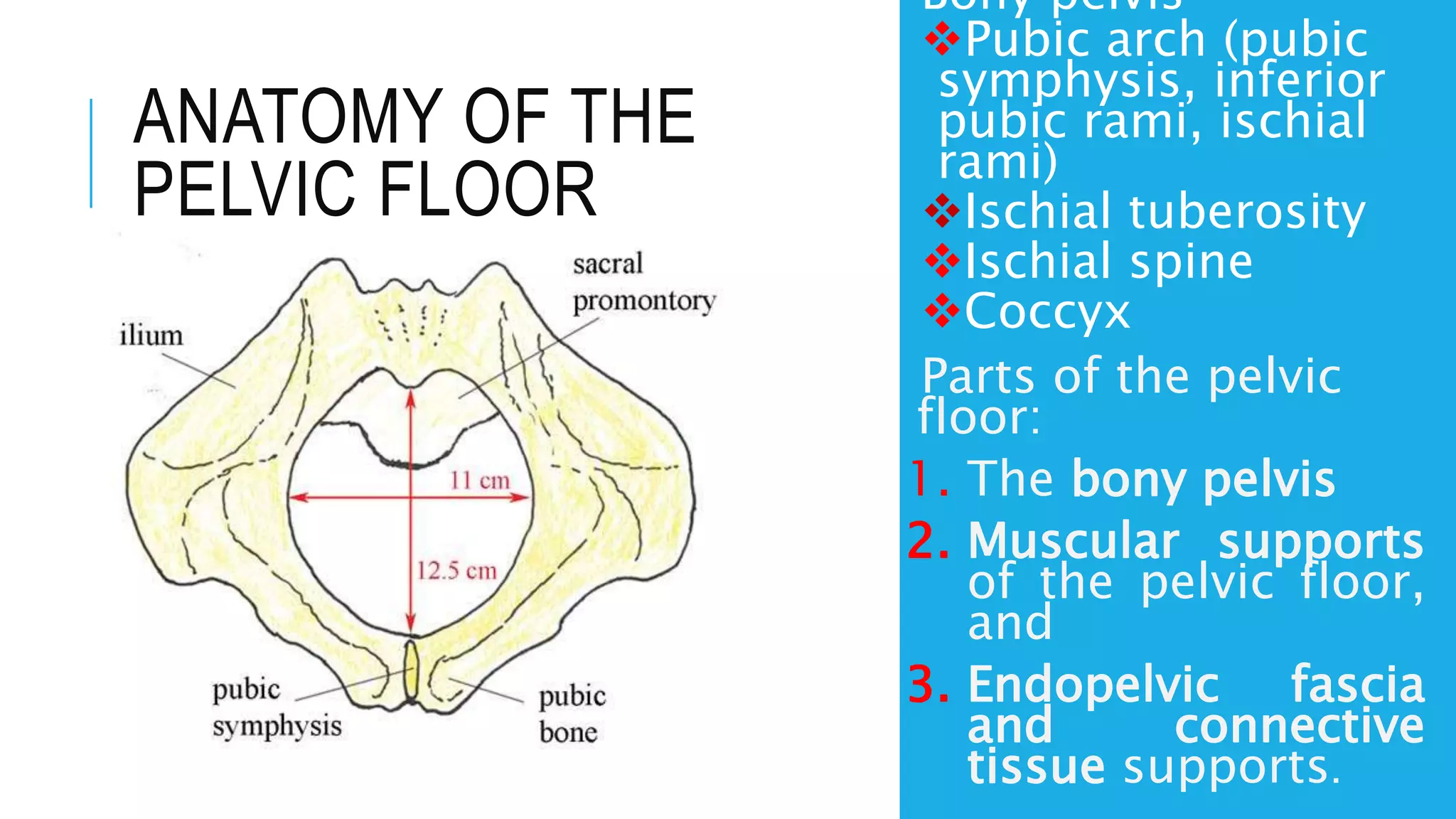
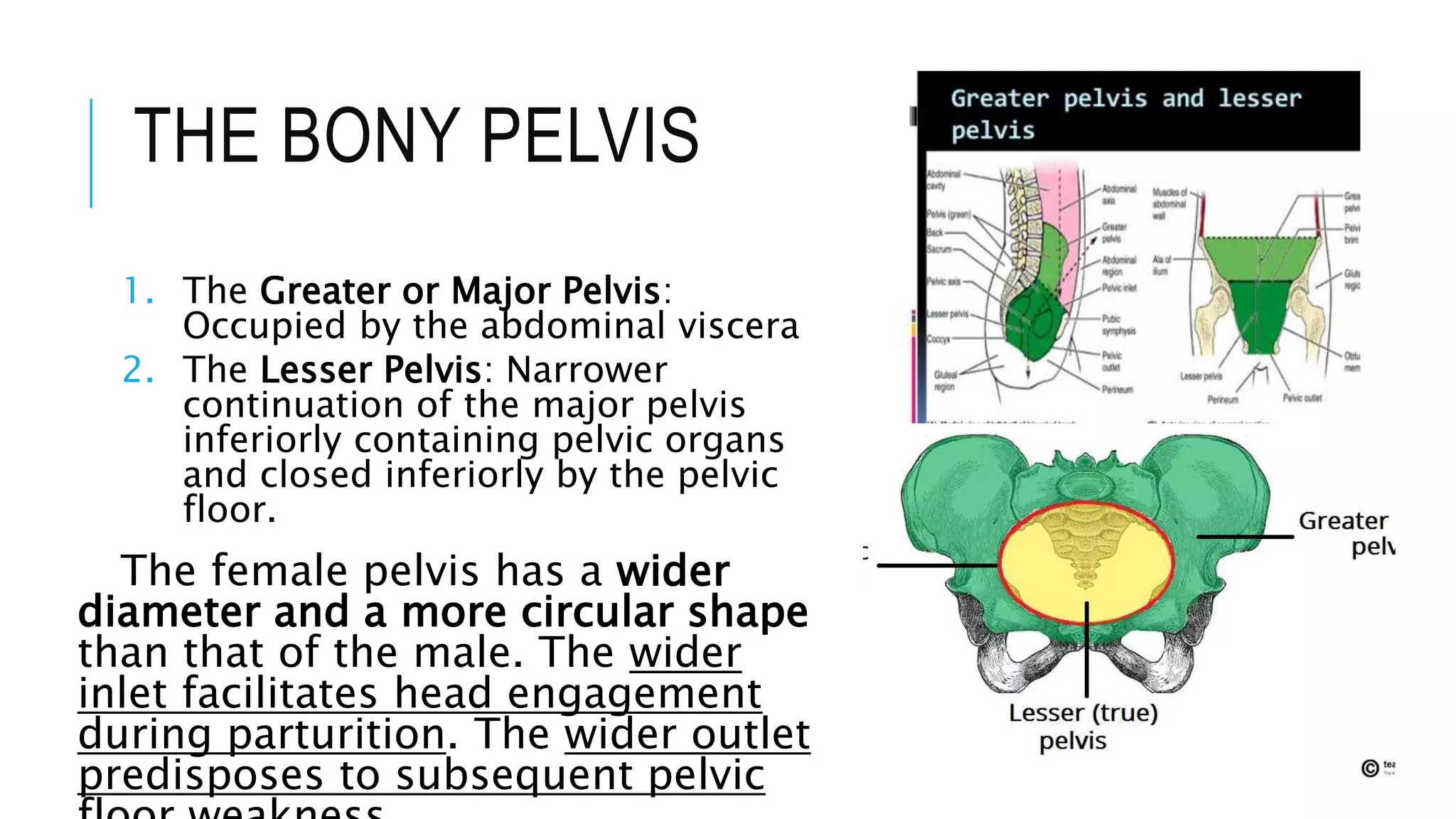
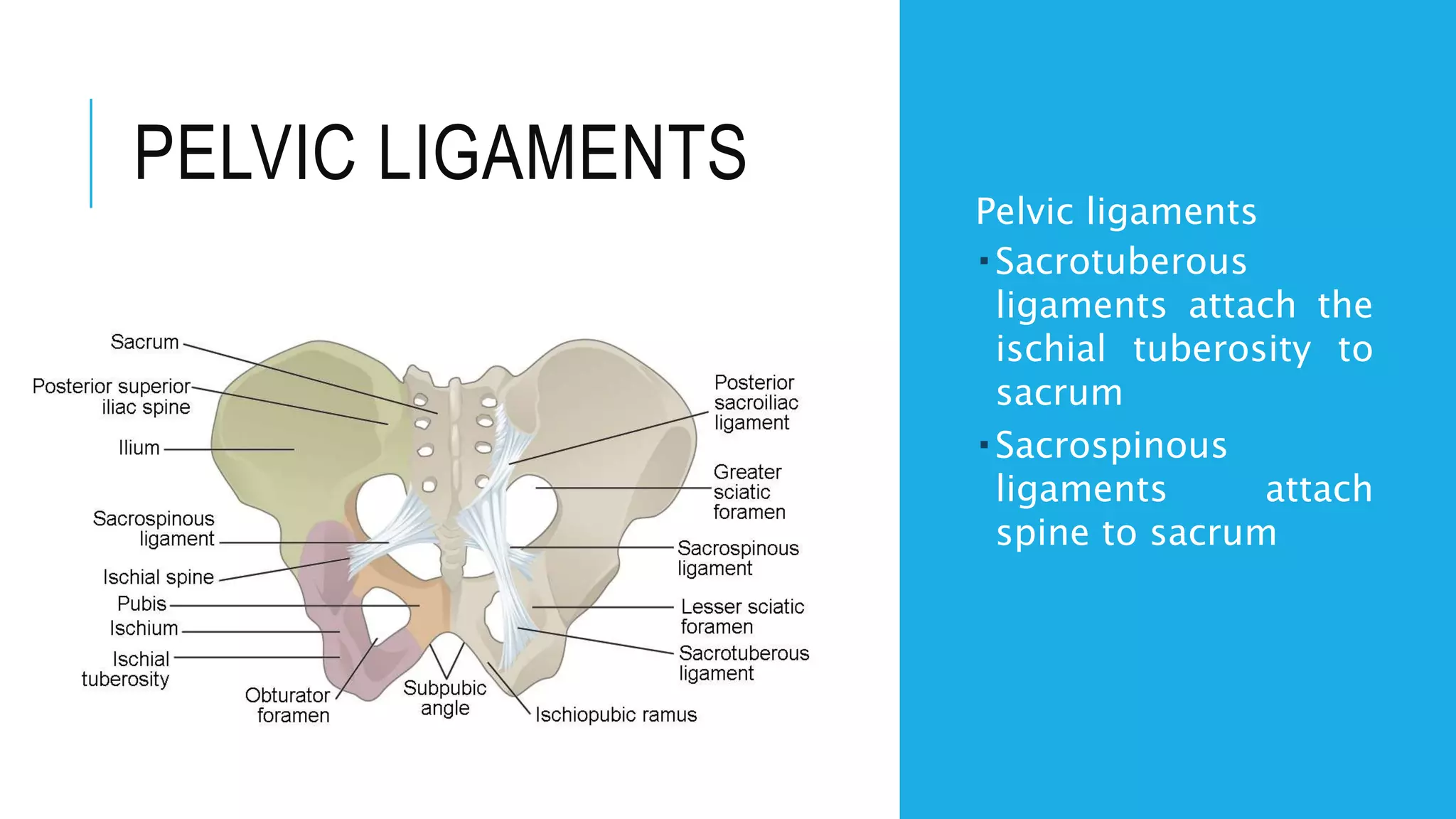
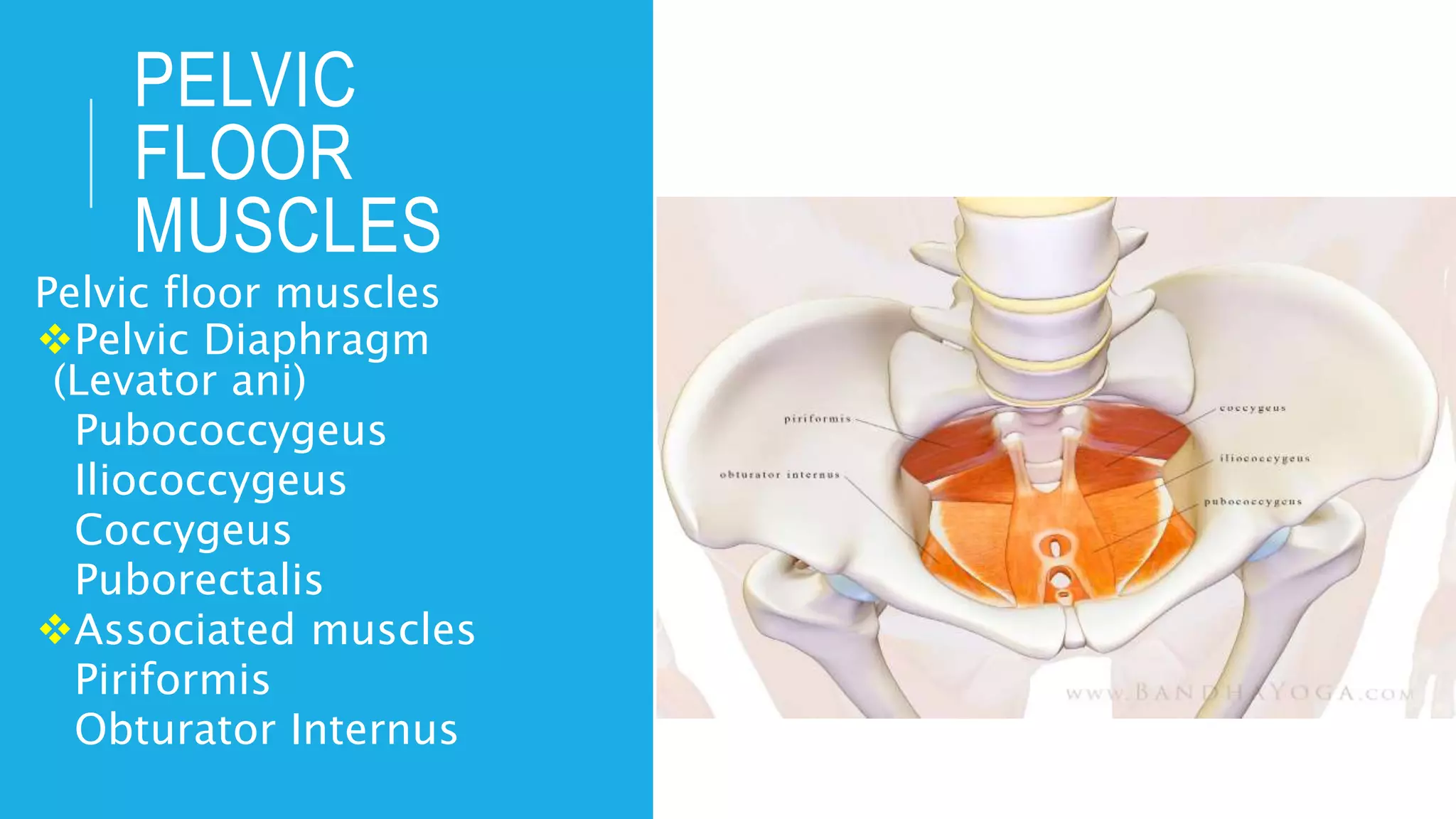
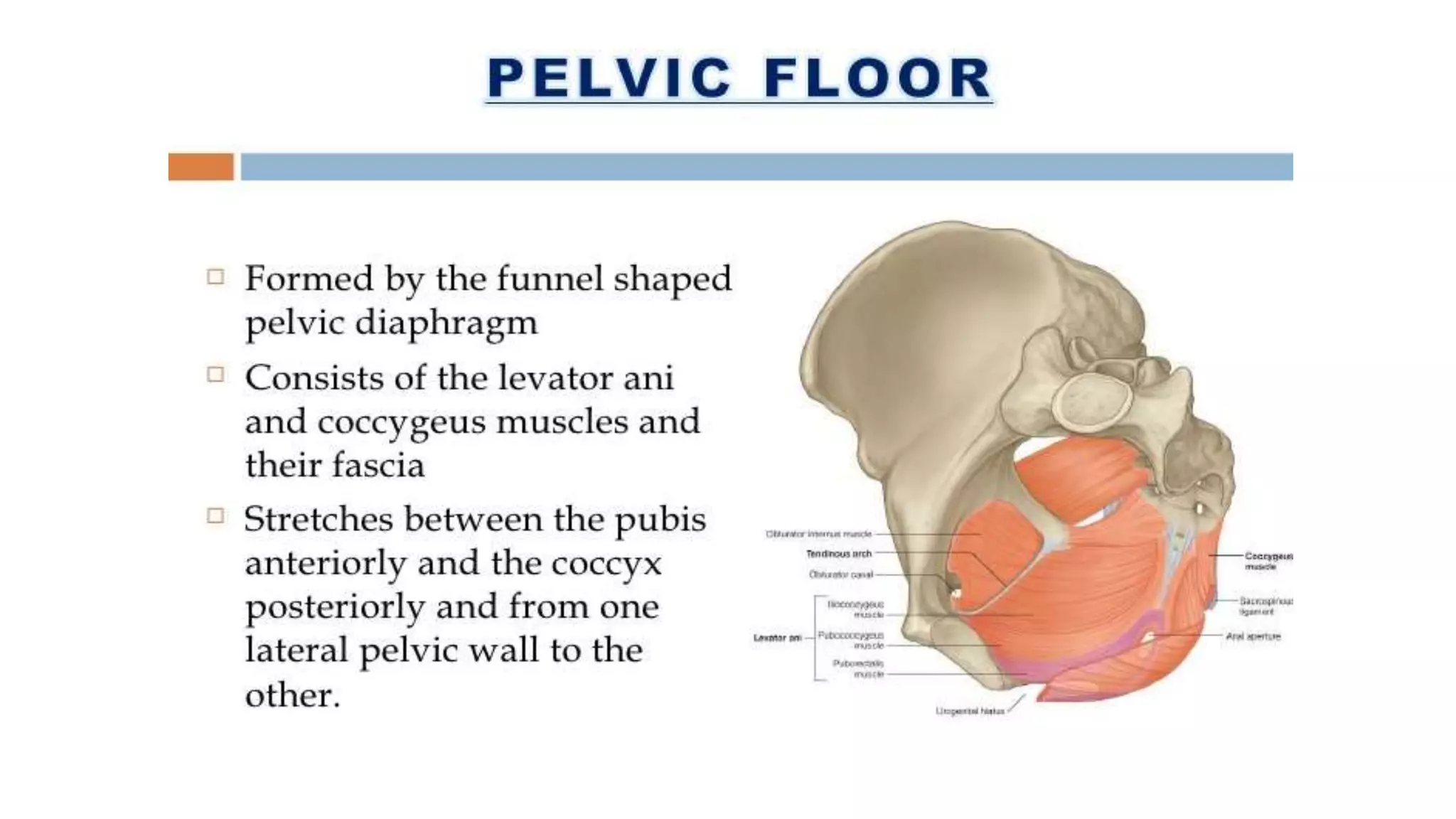
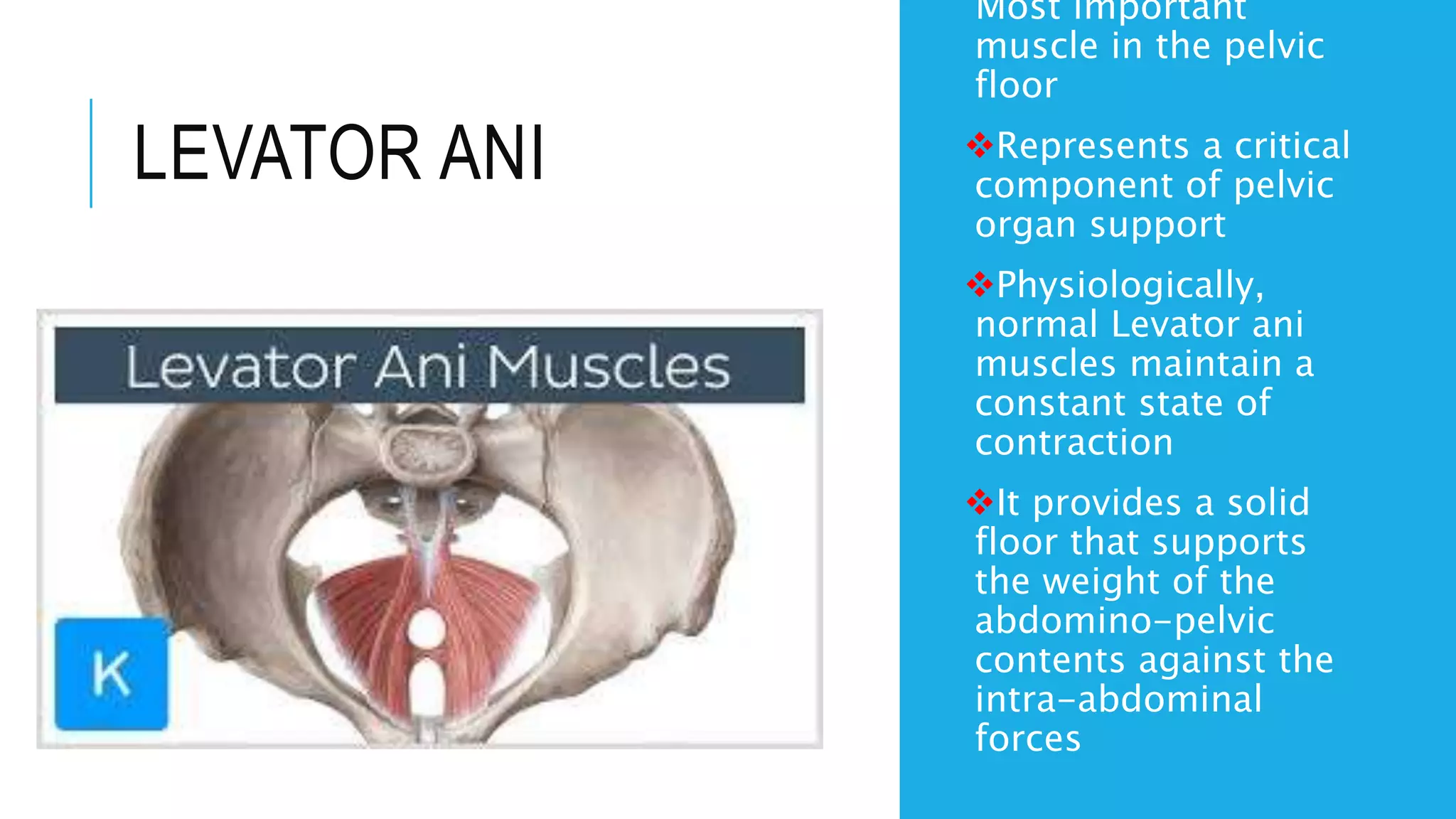
The document provides a comprehensive overview of the anatomy and function of the female pelvic floor, detailing its structure including the bony pelvis, pelvic floor muscles, and associated connective tissues. It discusses the importance of pelvic floor muscles in supporting pelvic organs, the effects of pregnancy and childbirth, and conditions that may necessitate pelvic floor physiotherapy. Additionally, it outlines therapeutic goals and interventions for improving pelvic floor function, such as exercises and educational strategies to enhance continence and alleviate pain.