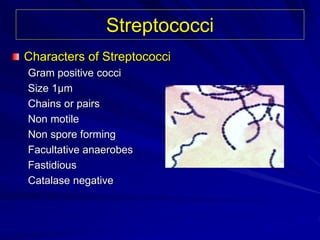
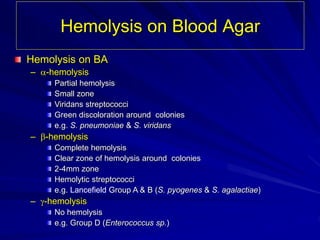
The document describes the characteristics and classification of streptococci, including their morphology, hemolytic properties, and Lancefield classification. It details diseases caused by Streptococcus pyogenes, including suppurative and toxin-mediated infections, and non-suppurative complications such as rheumatic fever. The document also outlines the diagnostic methods and treatment options for streptococcal infections.