1. Digital subtraction angiography (DSA) is an X-ray procedure that involves acquiring digital fluoroscopic images before and after injecting contrast dye and digitally subtracting the pre-contrast images from the post-contrast images, clearly showing blood vessels.
2. Proper pre-procedural preparation includes obtaining consent, checking vitals, performing imaging like CTA, and ensuring proper anticoagulation. Instruments used include access needles, guidewires, and dilators to facilitate catheter entry into vessels.
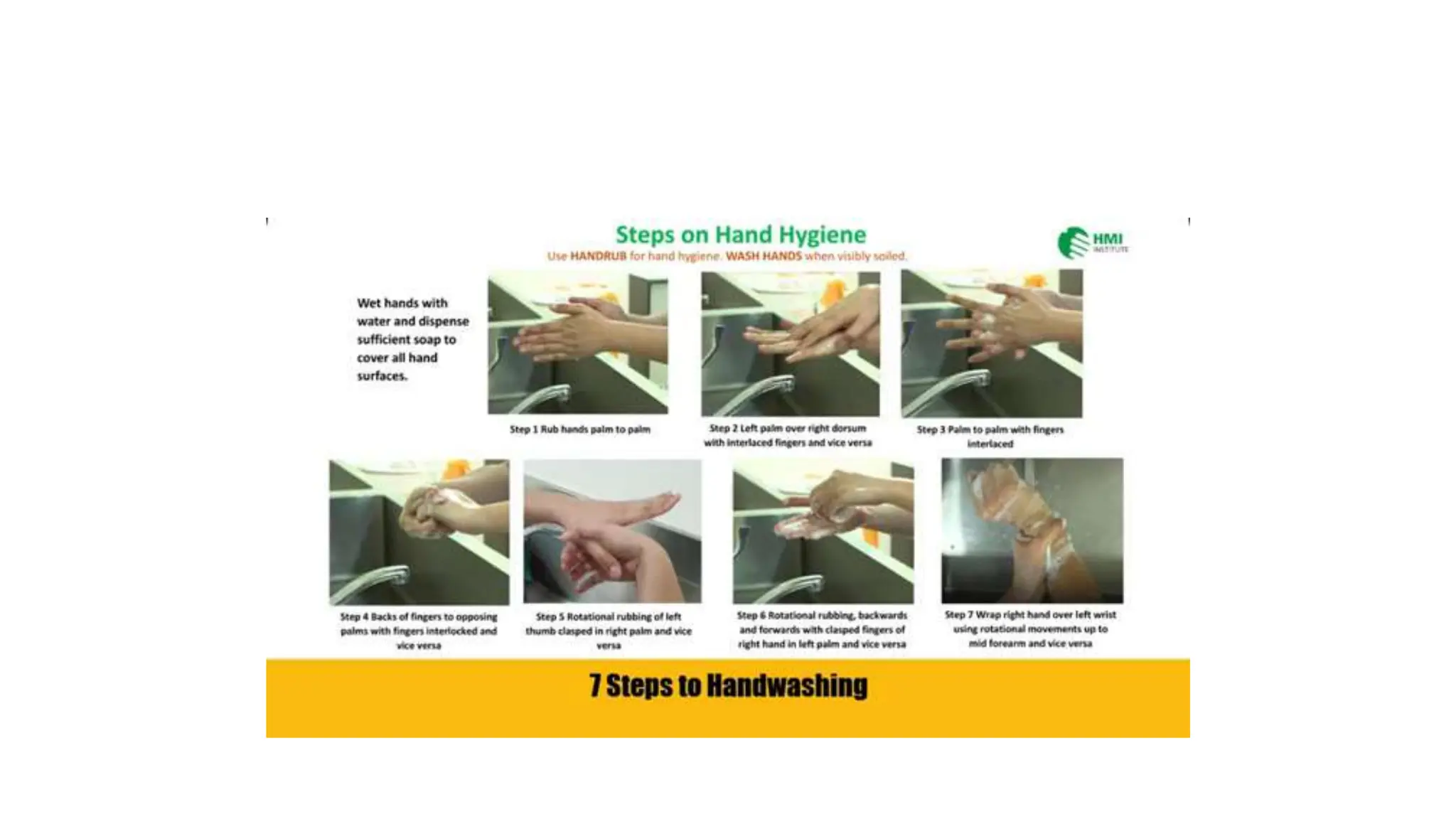
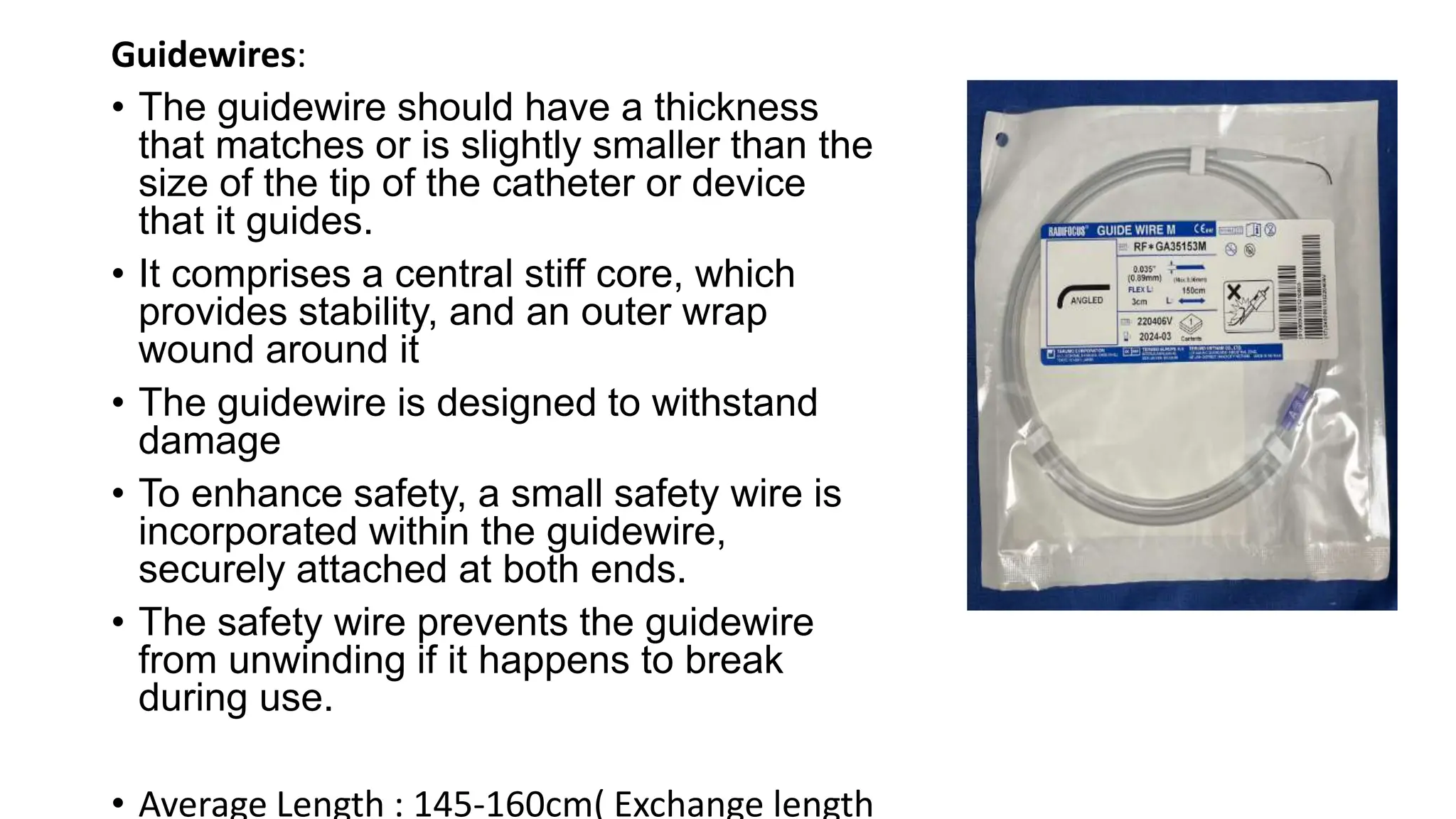
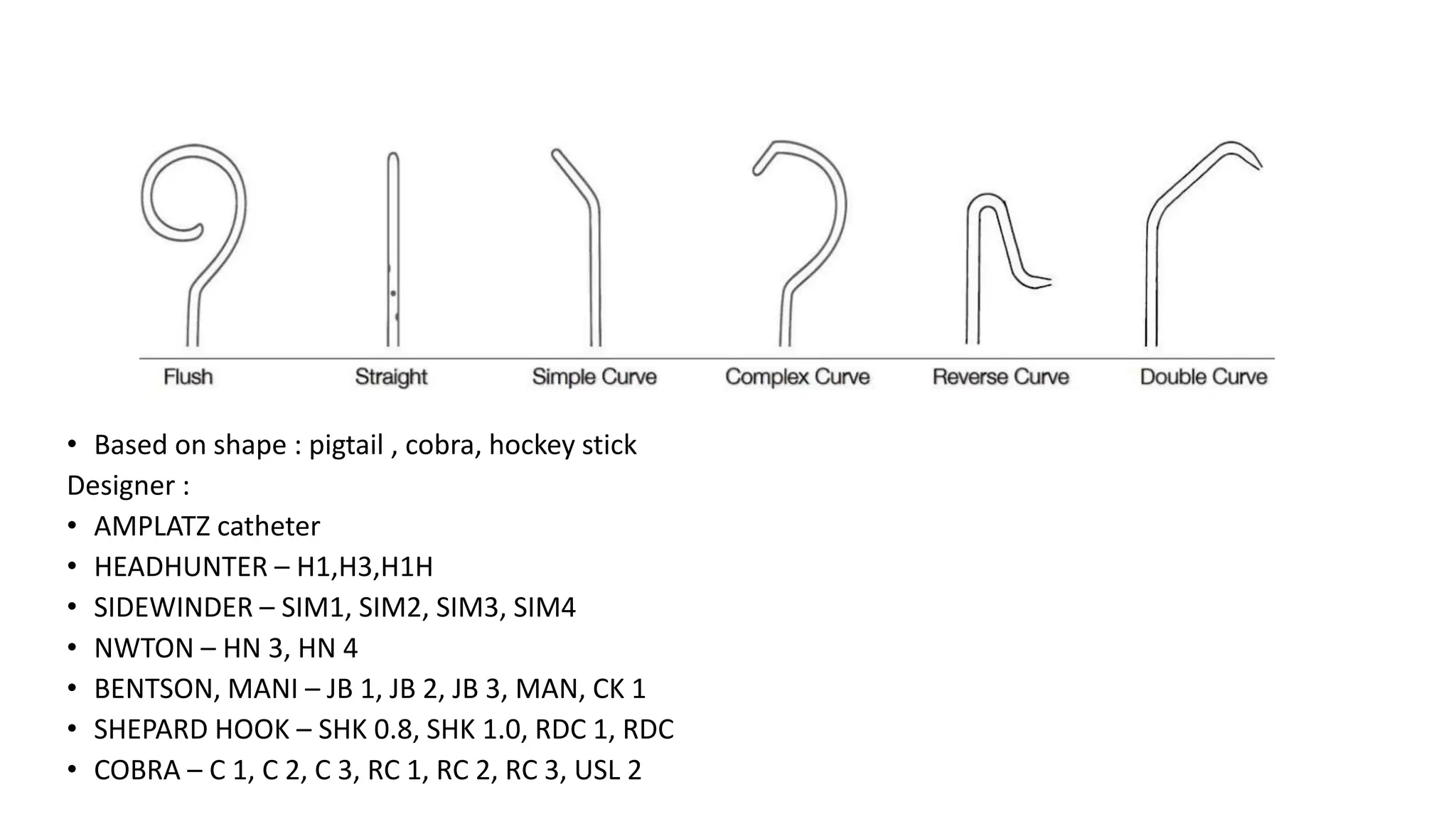
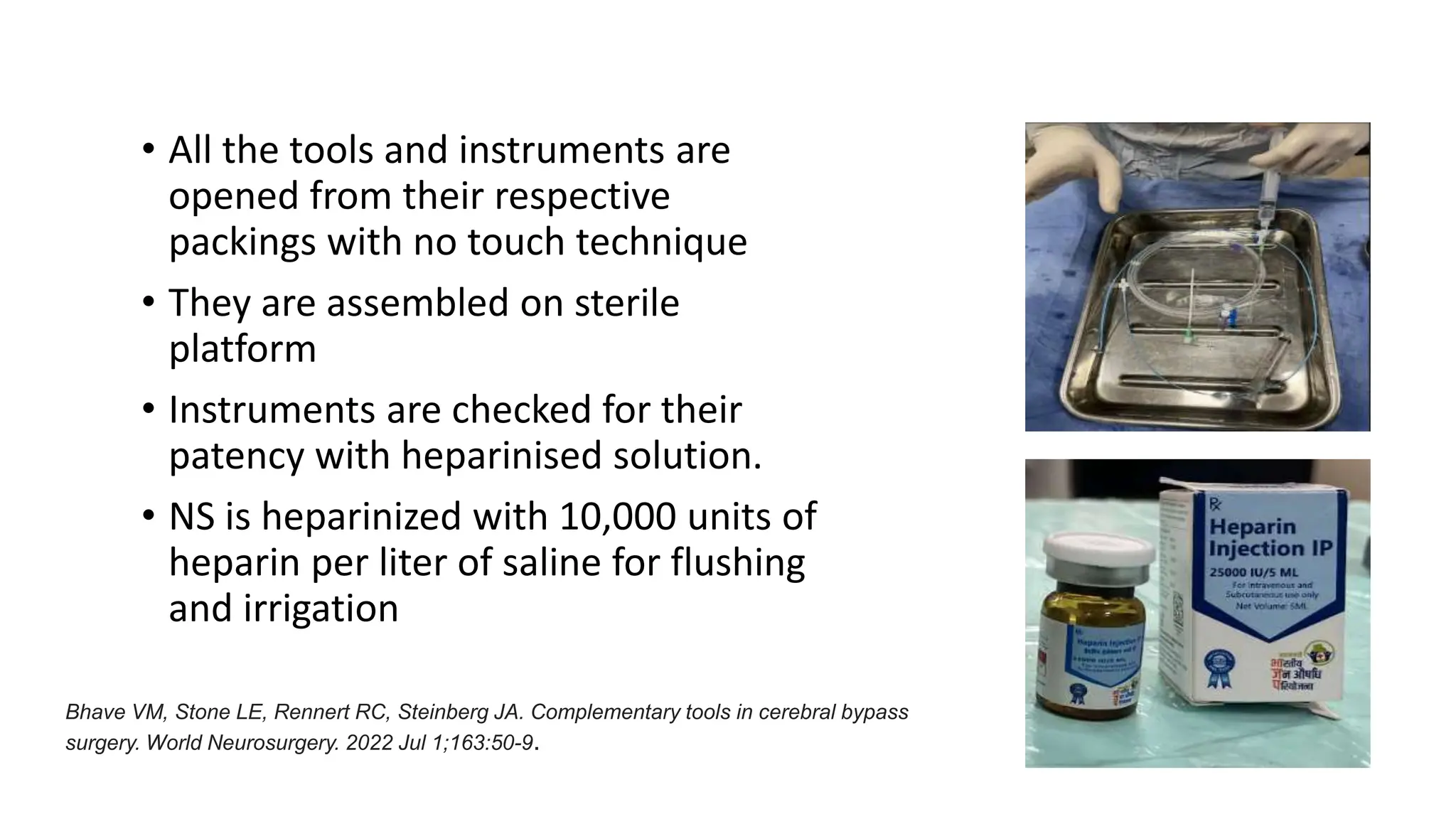
3. Strict aseptic techniques like appropriate skin antisepsis, sterile draping, and instrument sterilization are followed to prevent infections at the puncture site.