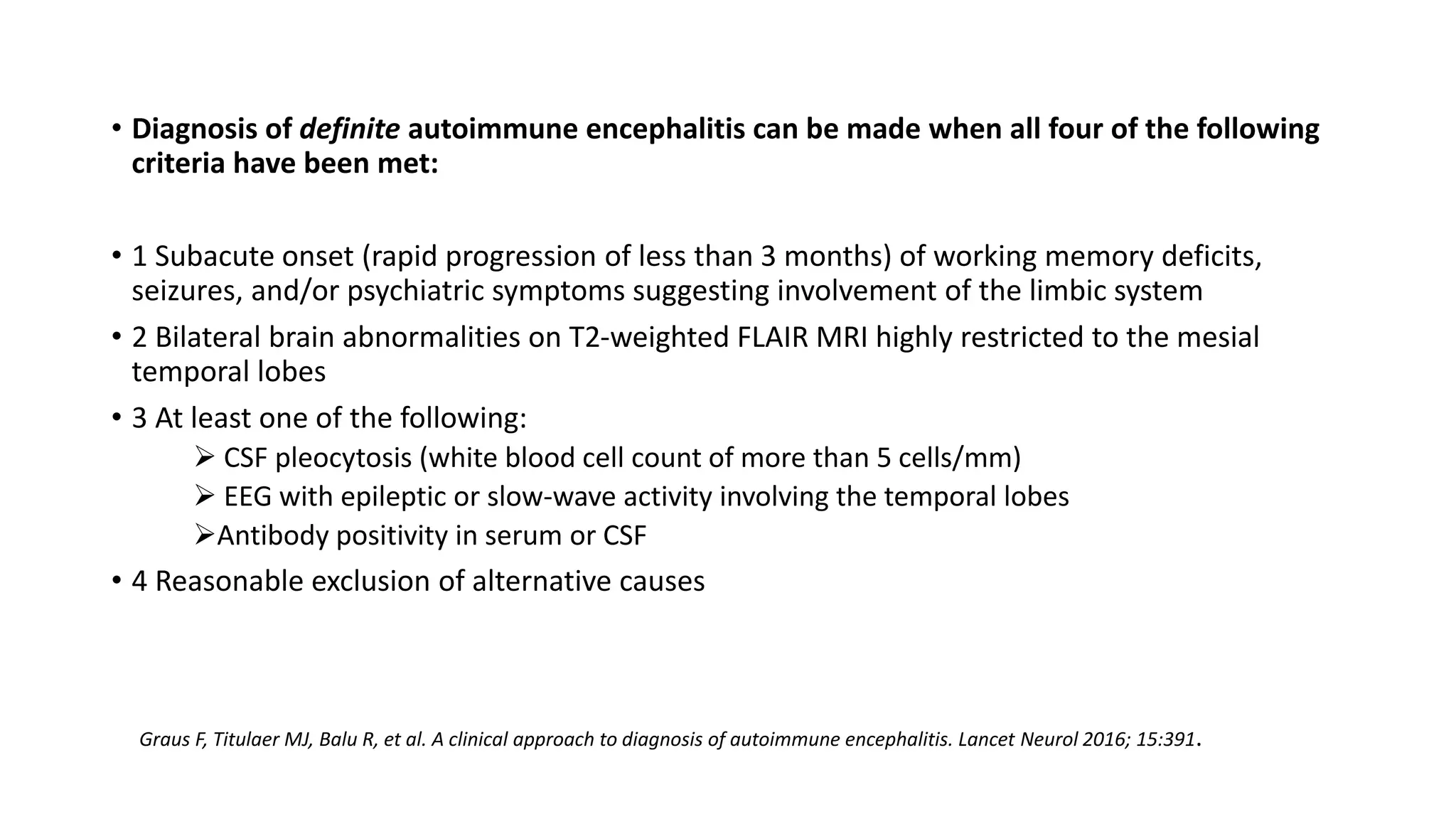
This document outlines treatment protocols for anti-NMDA and anti-LGI1 receptor encephalitis. It discusses diagnostic criteria for autoimmune encephalitis and provides clues to an autoimmune etiology. For anti-NMDA receptor encephalitis, it details diagnostic criteria and management, including first line treatment with corticosteroids, IVIG, and plasma exchange. Rituximab and cyclophosphamide are second line therapies. Maintenance therapy may include corticosteroids, IVIG, or rituximab every 6 months to prevent relapse.


























![Largest study till date…..
• The largest single study on treatment and outcomes in anti-NMDA receptor encephalitis is a
retrospective study of 577 patients that included 501 patients for whom treatment effects and outcome
were assessable [8].
• Nearly all patients (94 percent) were treated with tumor removal and first-line immunotherapy,
including steroids, IVIG, and/or plasma exchange. Half of patients improved within the first four weeks
of first-line therapy.
• Of these, 97 percent had a good outcome at 24-month follow-up.
• Of the 221 patients who did not improve within the first four weeks of first-line therapy, 125 (57
percent) received rituximab, cyclophosphamide, or both. Patients who received second-line therapy
had a higher likelihood of a good outcome (modified Rankin Scale [mRS] 0 to 2) than those who did not
(odds ratio [OR] 2.7, 95% CI 1.2-5.8). Response rates were similar in adults and children.
• By 24 months, approximately 80 percent of patients achieved a good outcome (mRS 0 to 2) and 30
patients had died. Outcomes continued to improve for up to 18 months after symptom onset
• Twelve percent of patients relapsed within the first two years of the initial episode. Patients without a
tumor and those who did not receive second-line immunotherapy were at increased risk for relapse.
Titulaer MJ, McCracken L, Gabilondo I, et al. Treatment and prognostic factors for longterm outcome in patients with anti-NMDA
receptor encephalitis: an observational cohort study. Lancet Neurol 2013; 12:15](https://image.slidesharecdn.com/sumeetantinmda-copy-230415143513-a414a8eb/75/anti-NMDA-receptor-encephalitis-Copy-pptx-30-2048.jpg)








![• This [18F]fluorodeoxyglucose (FDG) PET study evaluates the accuracy of semiquantitative
measurement of Putaminal hypermetabolism in identifying anti–leucine-rich, glioma–
inactivated-1 (LGI1) protein autoimmune encephalitis (AE)
• Semiquantitative measurement of Putaminal hypermetabolism with FDG-PET may be used to
distinguish LGI1-AE from other pathologies
• Metabolic abnormalities in LGI1-AE also extend beyond putamen and MTL into other
subcortical and cortical regions
• FDG-PET may be used in evaluating disease evolution in LGI1-AE.
• Patients with good short-term outcome (mRS ≤ 2) at the time of follow-up PET showed a
reduction in MTL hypermetabolism .
Rissanen E, Carter K, Cicero S, Ficke J, Kijewski M, Park MA, Kijewski J, Stern E, Chitnis T, Silbersweig D, Weiner HL.
Cortical and subcortical dysmetabolism are dynamic markers of clinical disability and course in anti-LGI1 encephalitis.
Neurology-Neuroimmunology Neuroinflammation. 2022 Mar 1;9(2).](https://image.slidesharecdn.com/sumeetantinmda-copy-230415143513-a414a8eb/75/anti-NMDA-receptor-encephalitis-Copy-pptx-39-2048.jpg)






















































































