Downloaded 152 times
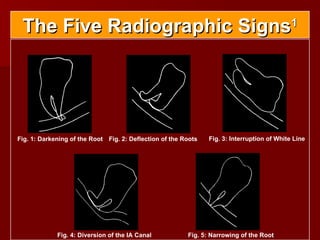
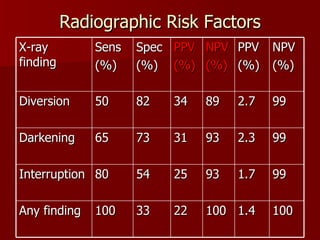



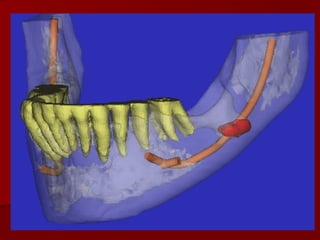
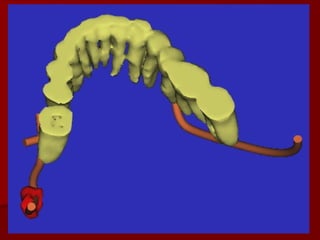
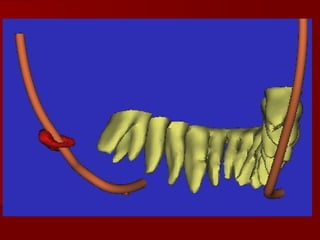


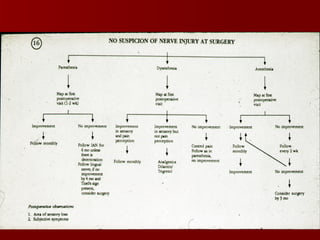
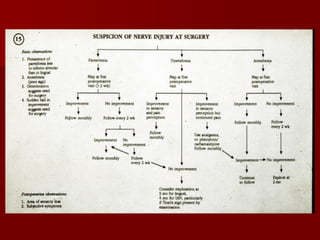

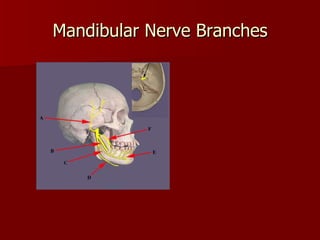
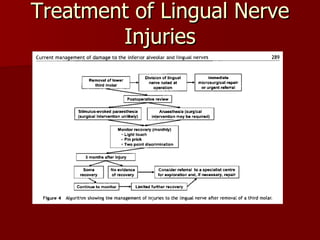


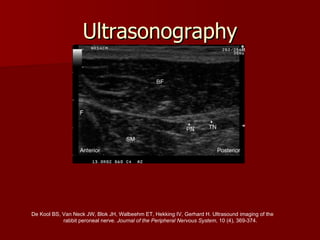

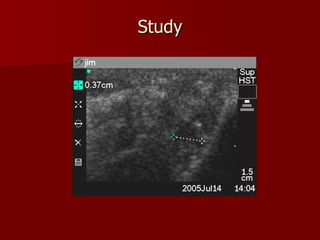
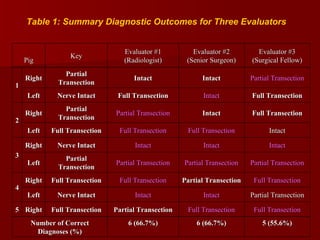
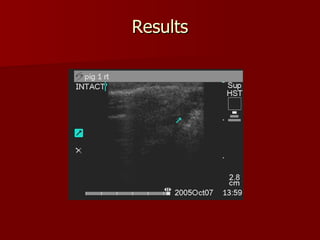
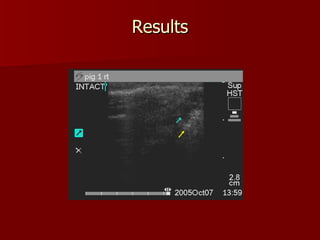
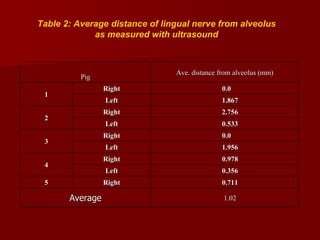




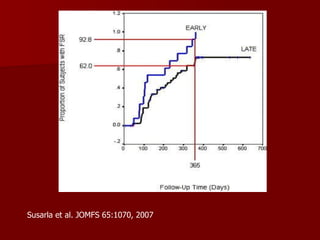
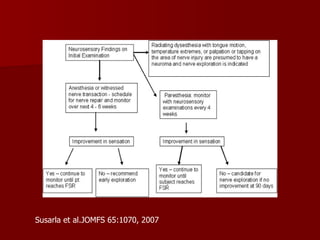
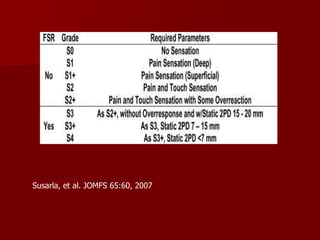
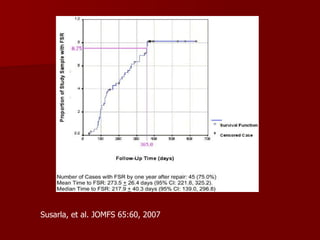


The document discusses algorithms for managing inferior alveolar and lingual nerve injuries, particularly in the context of various dental procedures. It covers diagnostic approaches, including ultrasound visualization of the lingual nerve, and the implications of different radiographic signs. Additionally, it highlights the need for further research to improve treatment outcomes and surgical planning for nerve injuries.








![Anatomical consideration for local anesthesia [innervation]](https://cdn.slidesharecdn.com/ss_thumbnails/anatomicalconsiderationforlocalanesthesiainnervation-120303015858-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)


































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)











