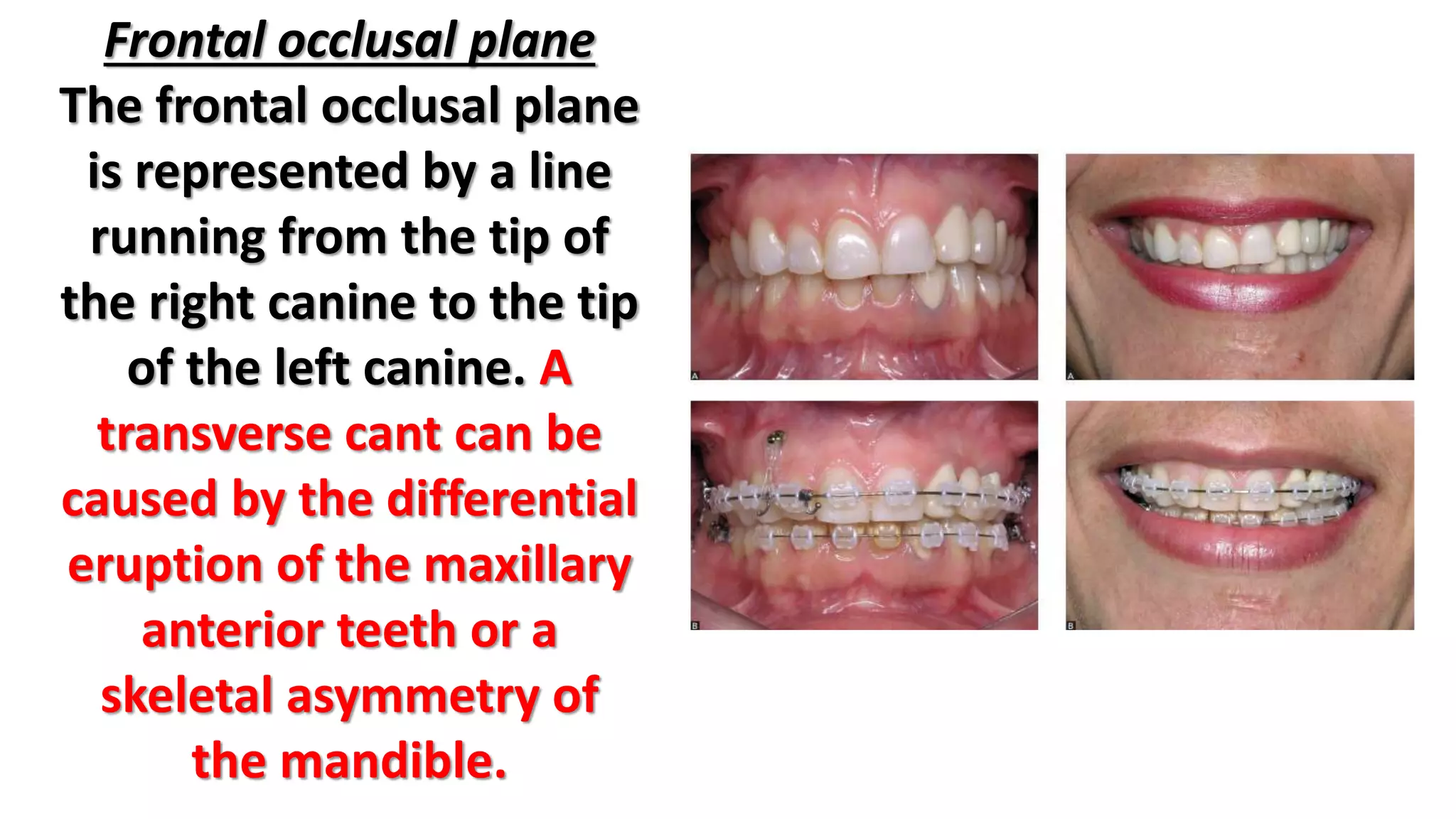
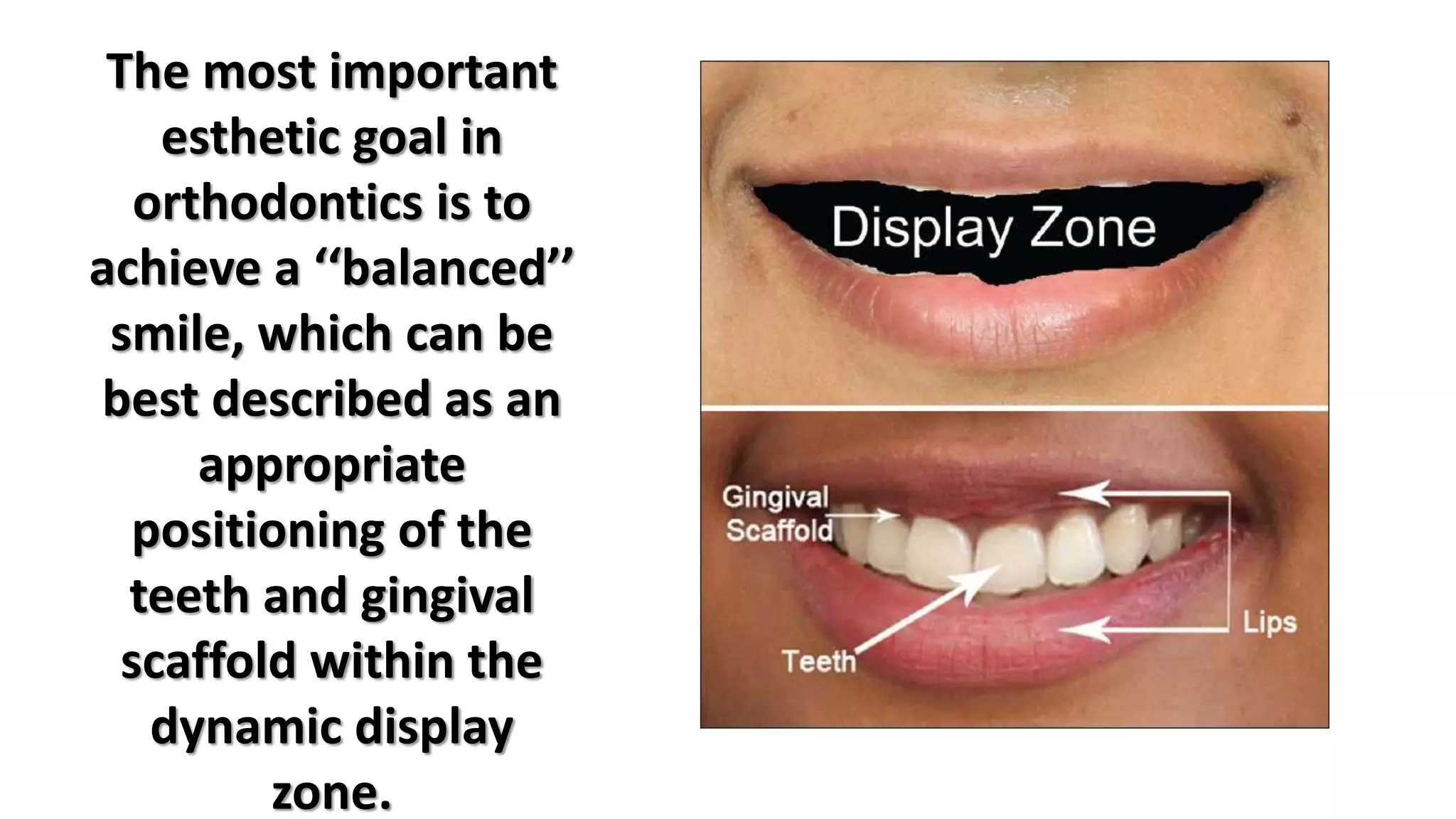
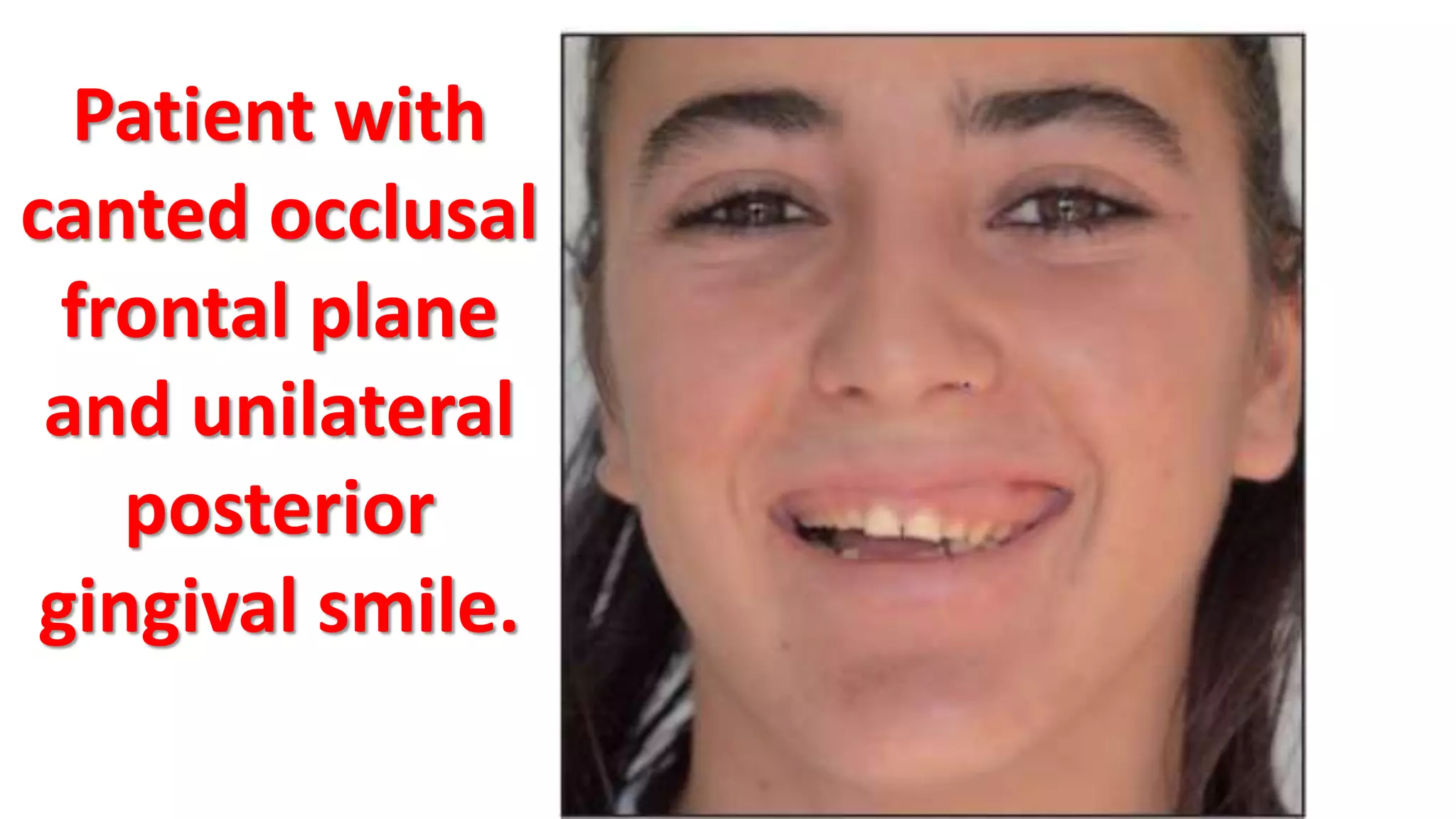
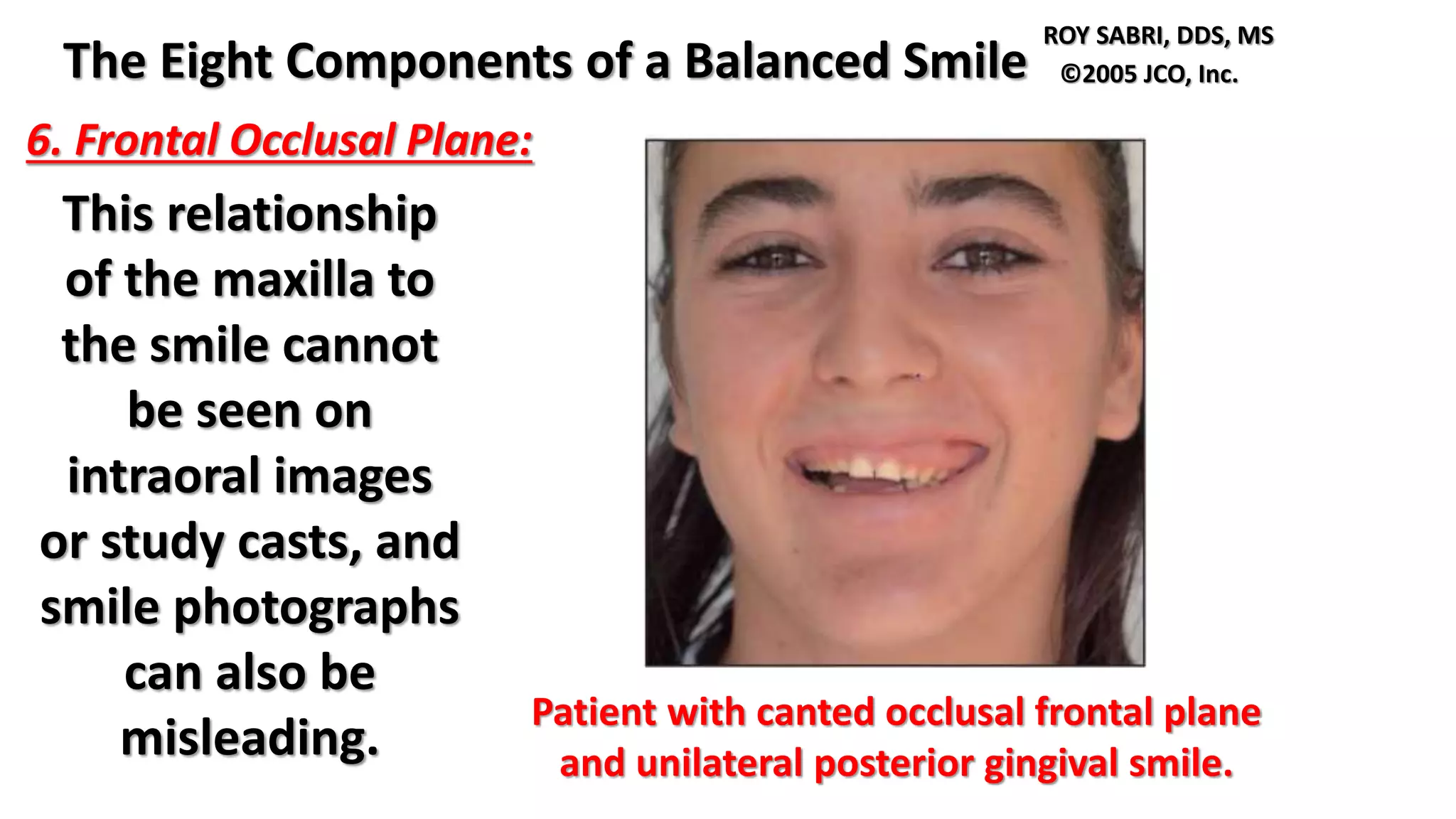
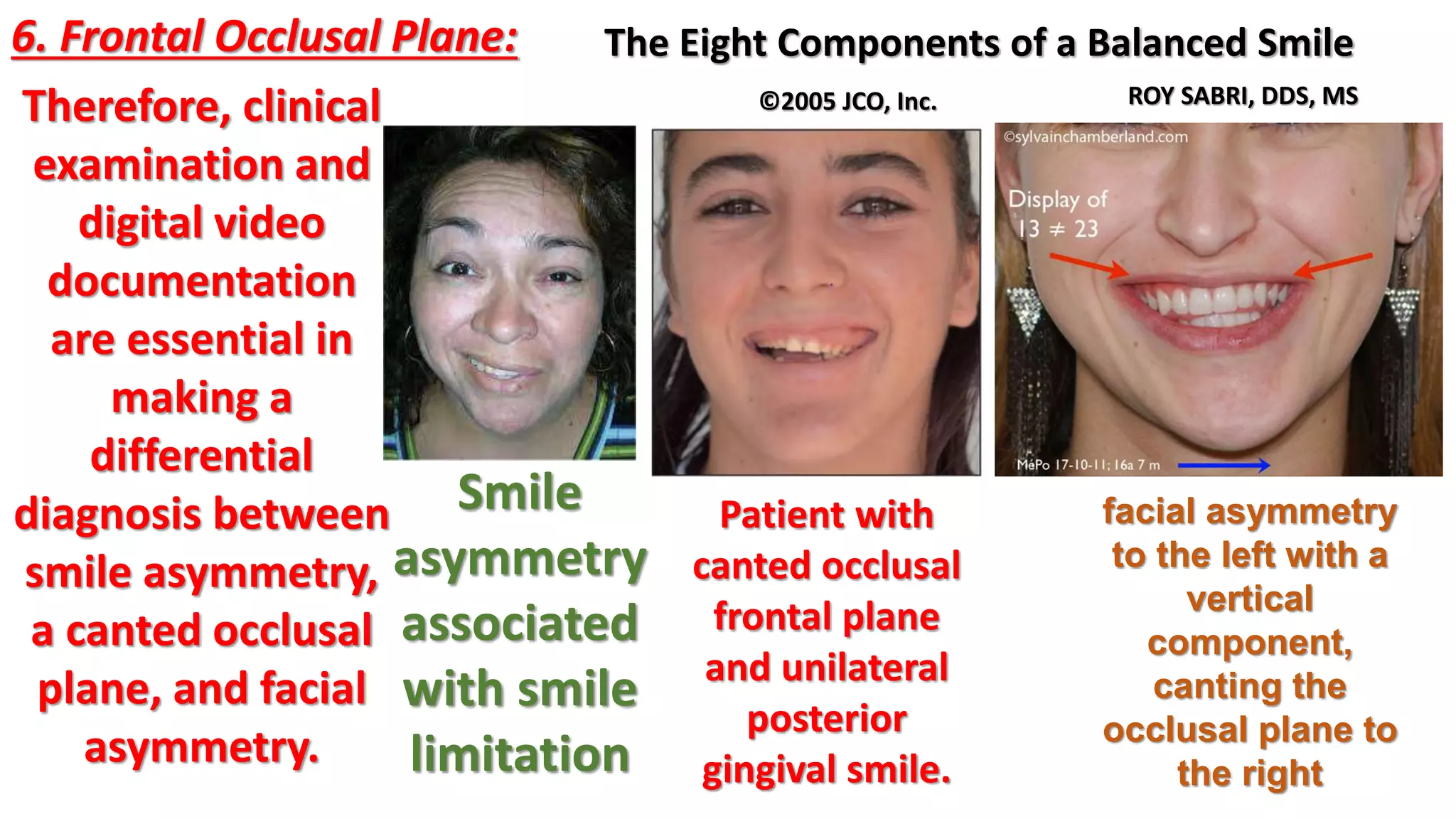
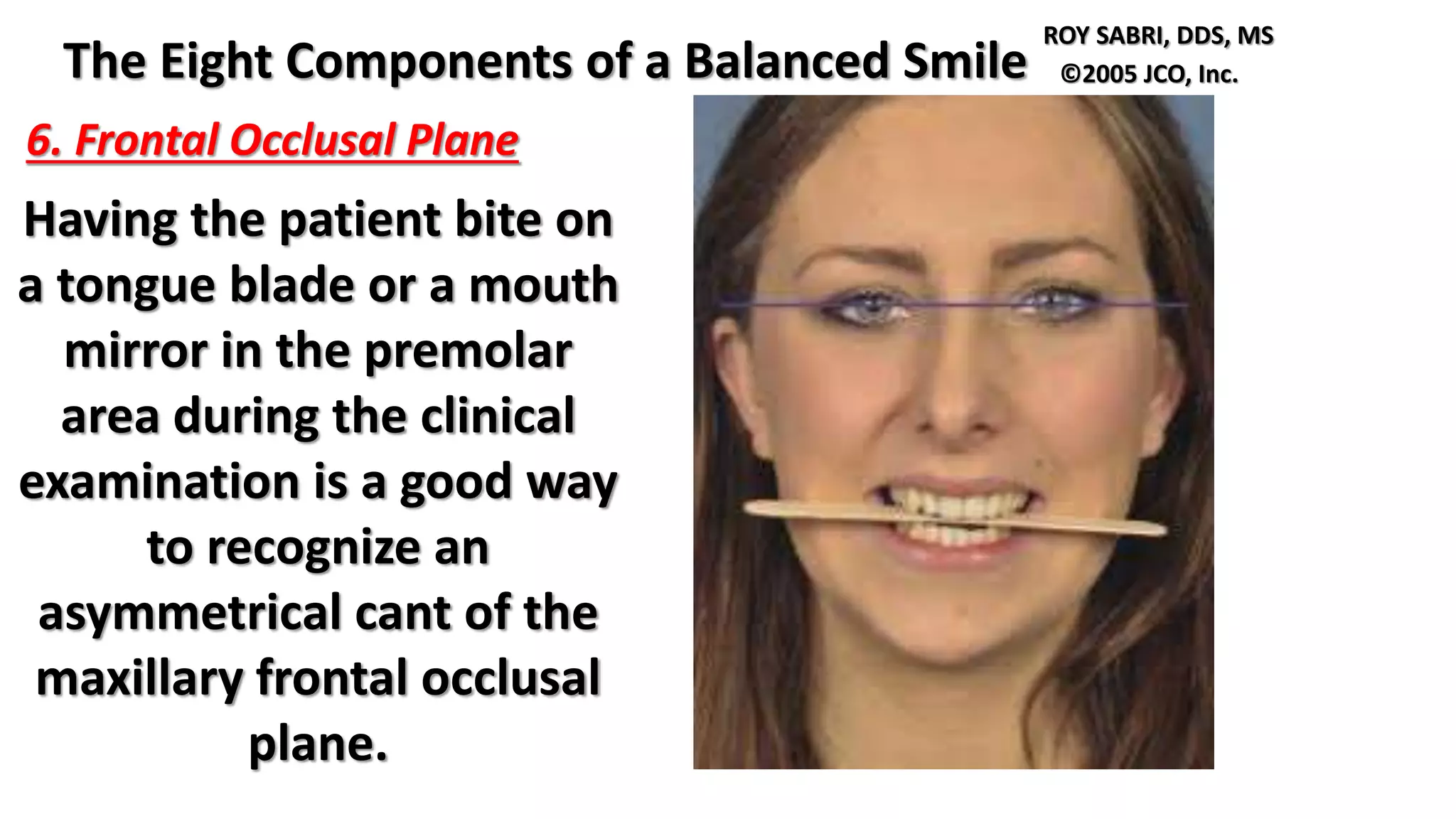
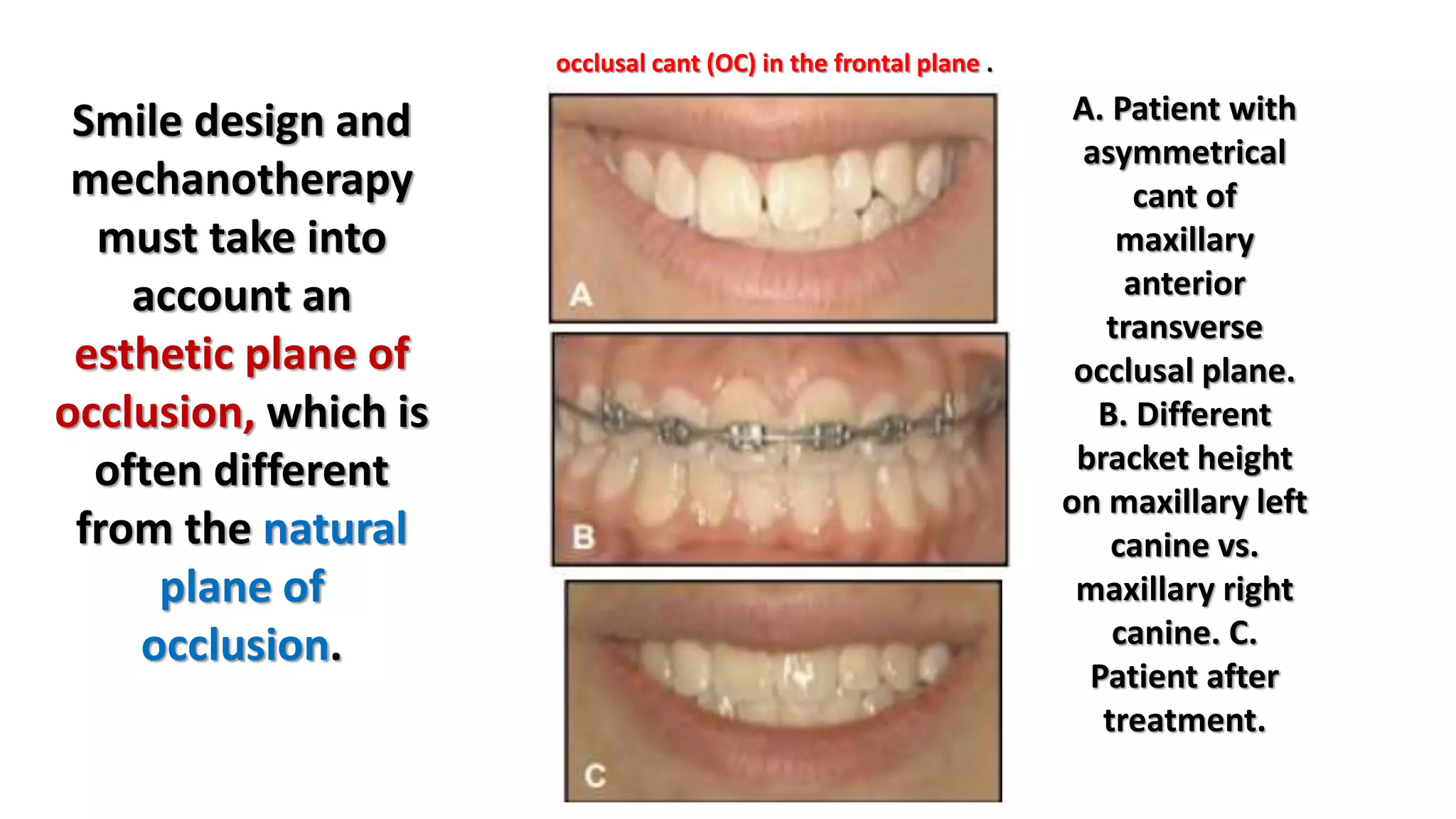
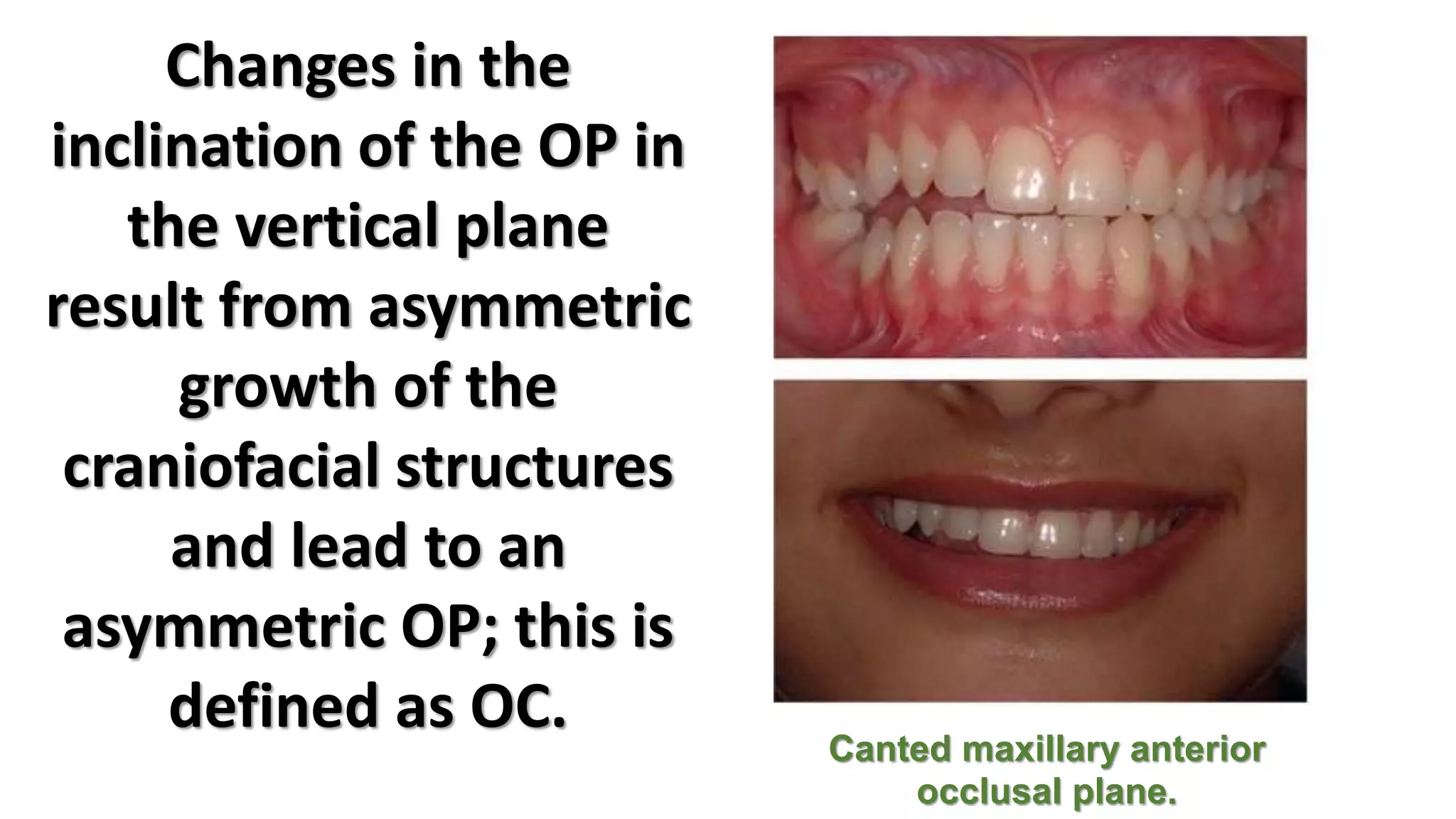
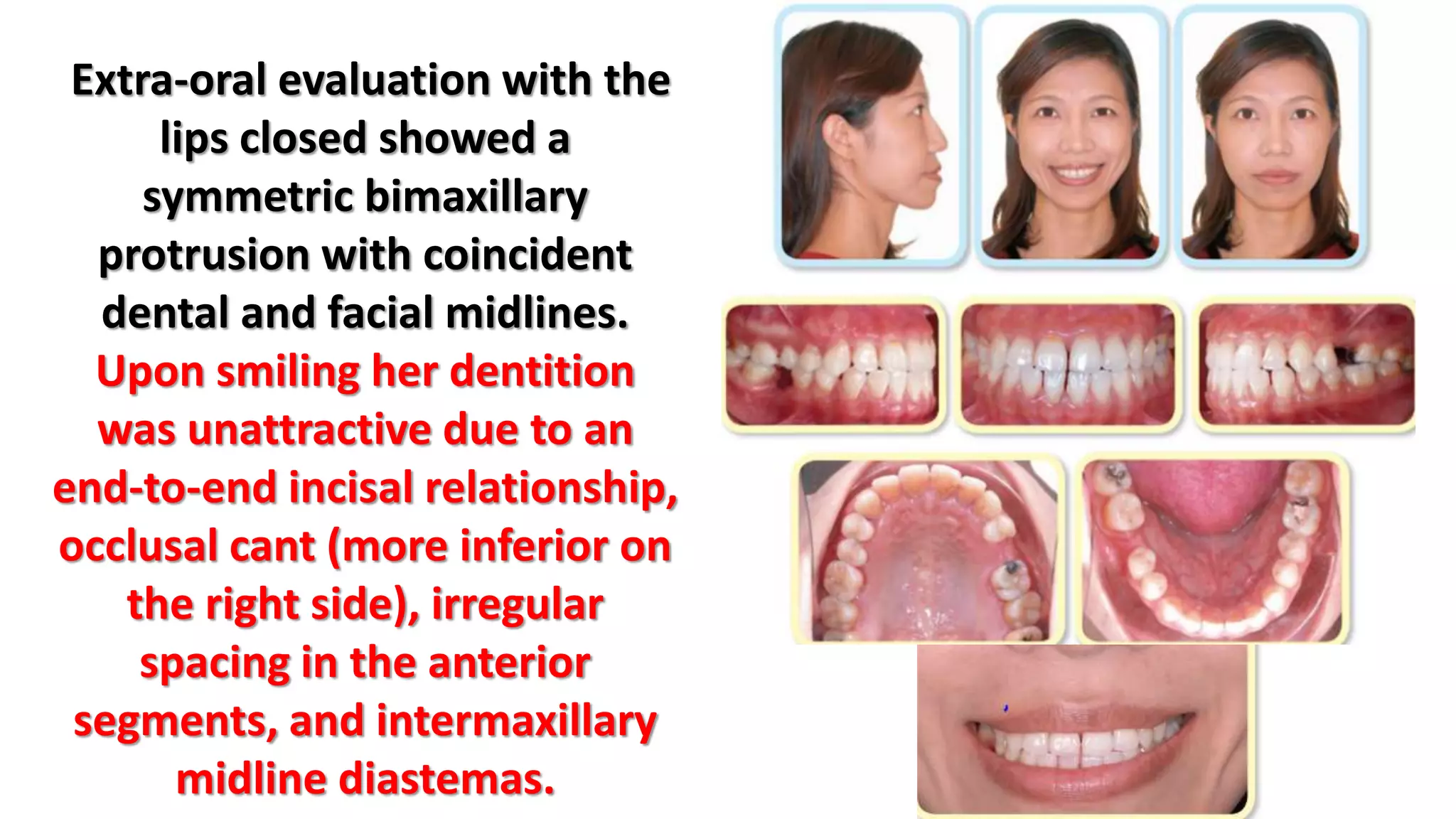
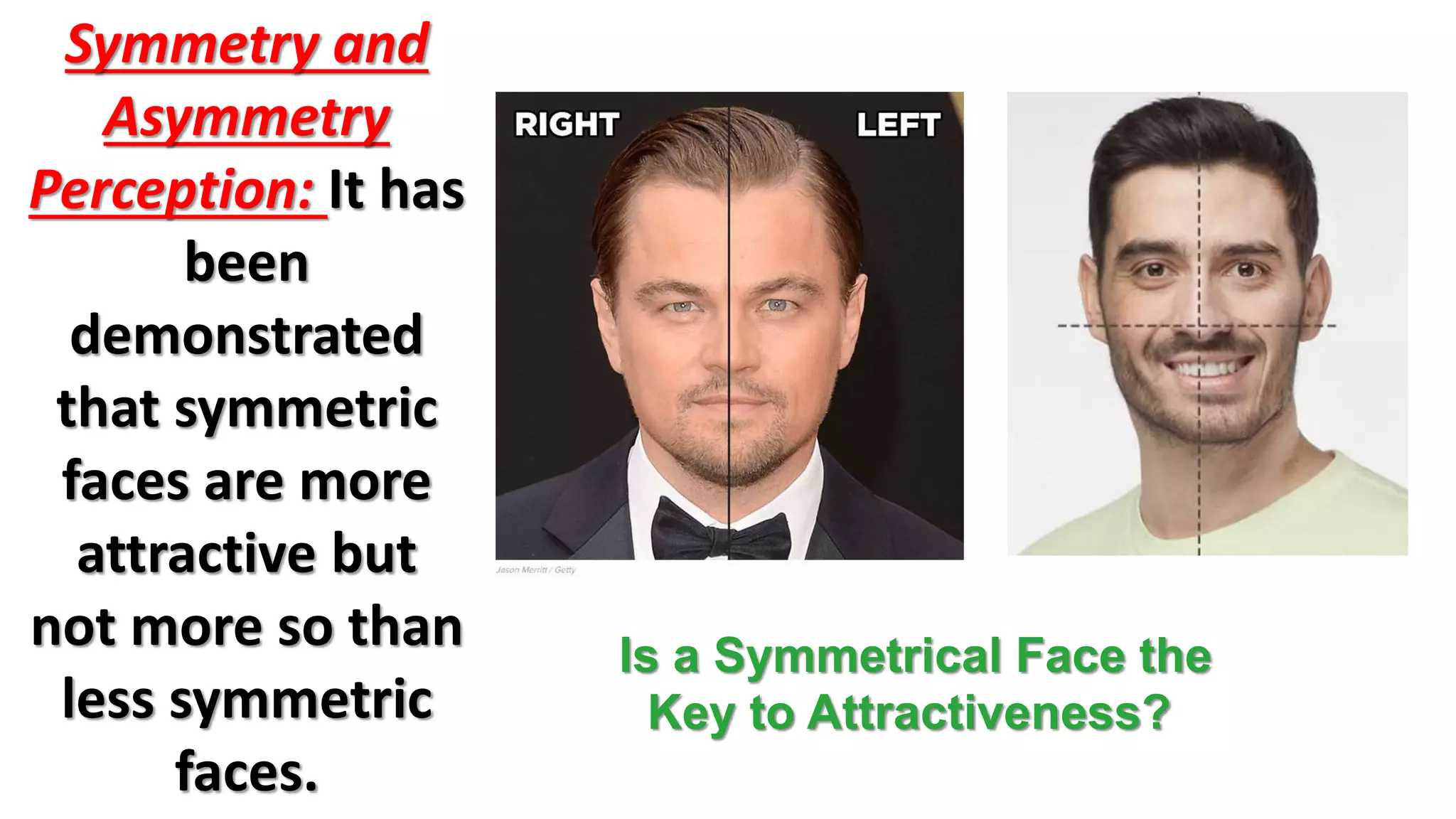
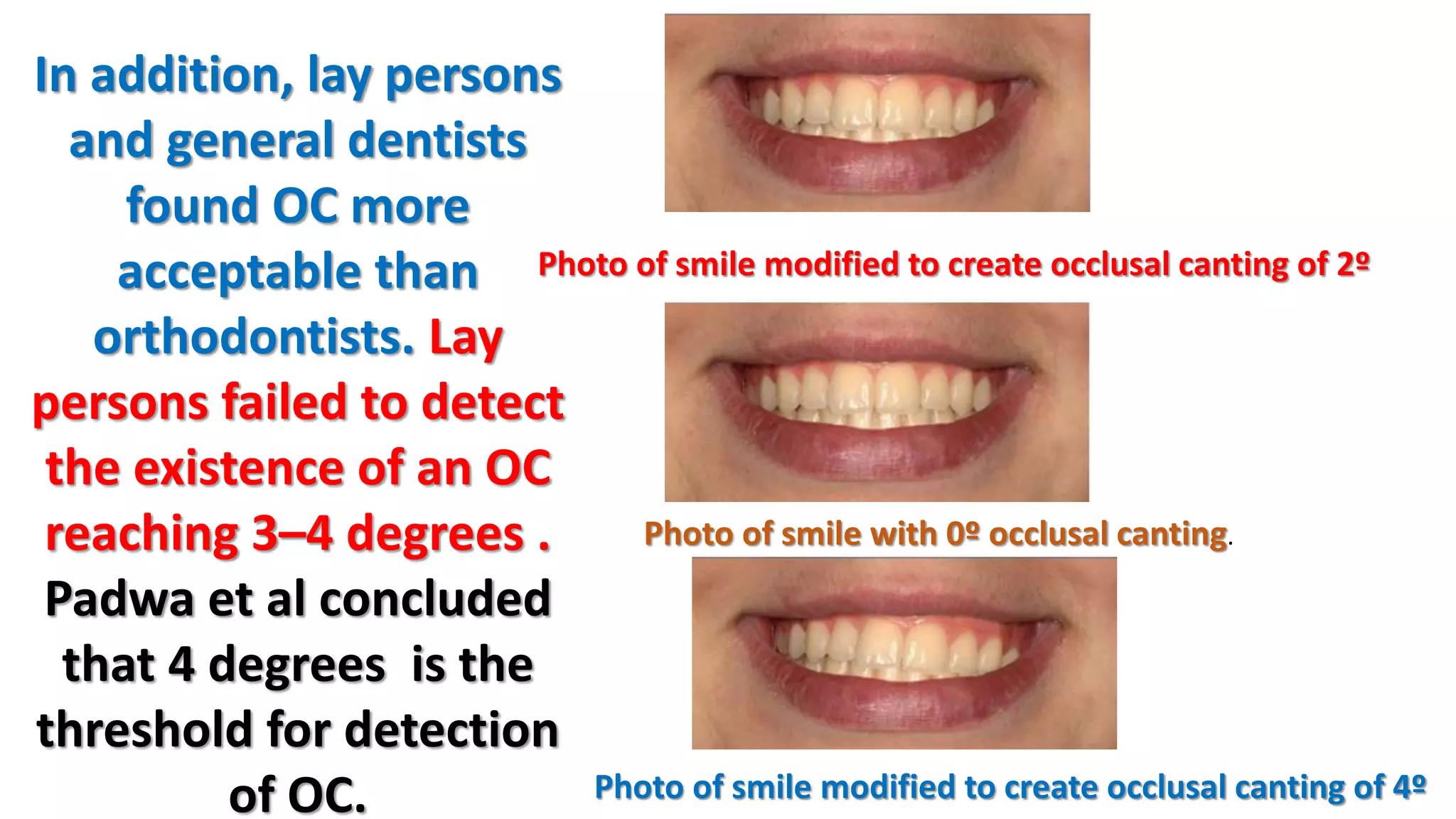
This document discusses canted occlusal planes, including their etiology, evaluation, and impact on smile esthetics. It provides details on how occlusal cant can result from asymmetric growth or positioning of dental arches. The perception and detection of occlusal cant varies, with 2-4 degrees generally considered acceptable. Both hereditary and environmental factors can contribute to asymmetries leading to occlusal canting. Proper evaluation involves clinical examination and documentation to differentiate cant from other potential causes like facial asymmetry or smile limitations.