Downloaded 23 times

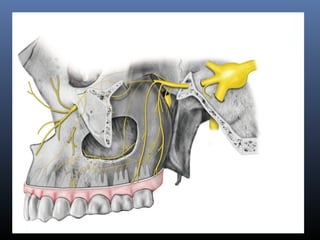
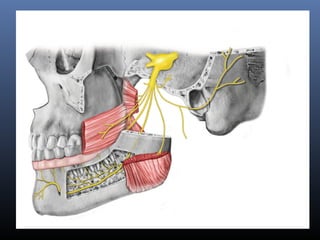
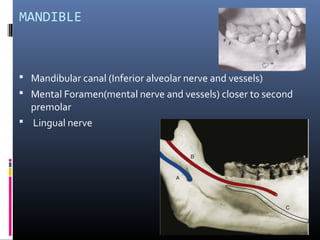
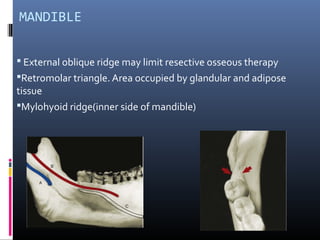
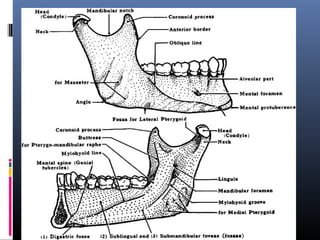


The document discusses the surgical anatomy of the periodontium and surrounding structures, emphasizing the importance of understanding these anatomical features for dental surgery. It details the anatomy of the mandible and maxilla, including crucial nerves and vessels, as well as relevant surgical spaces that can pose infection risks. Key cautions are highlighted for implant placement to avoid nerve damage and significant hemorrhage during procedures.























































































