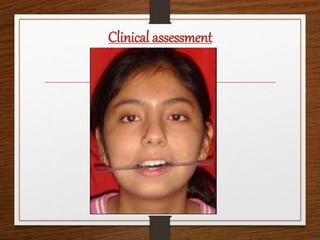
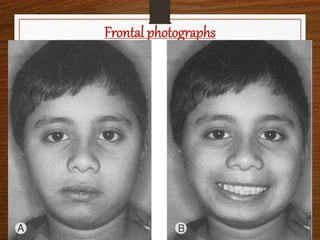
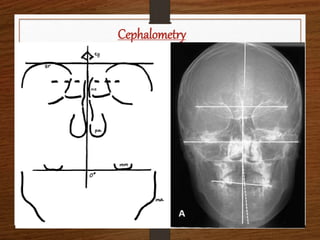
This document discusses the management of occlusal cant, which is asymmetry in the vertical inclination of the occlusal plane. It begins by defining occlusal cant and exploring its causes such as facial asymmetry or asymmetric growth. Methods for evaluating occlusal cant like clinical exams, photos, and imaging are presented. Treatment options include orthodontics using devices like bite blocks or orthodontic surgery to level the occlusal plane. The document concludes that both the etiology and classification of an individual's occlusal cant should be considered to determine the best treatment approach.














































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


