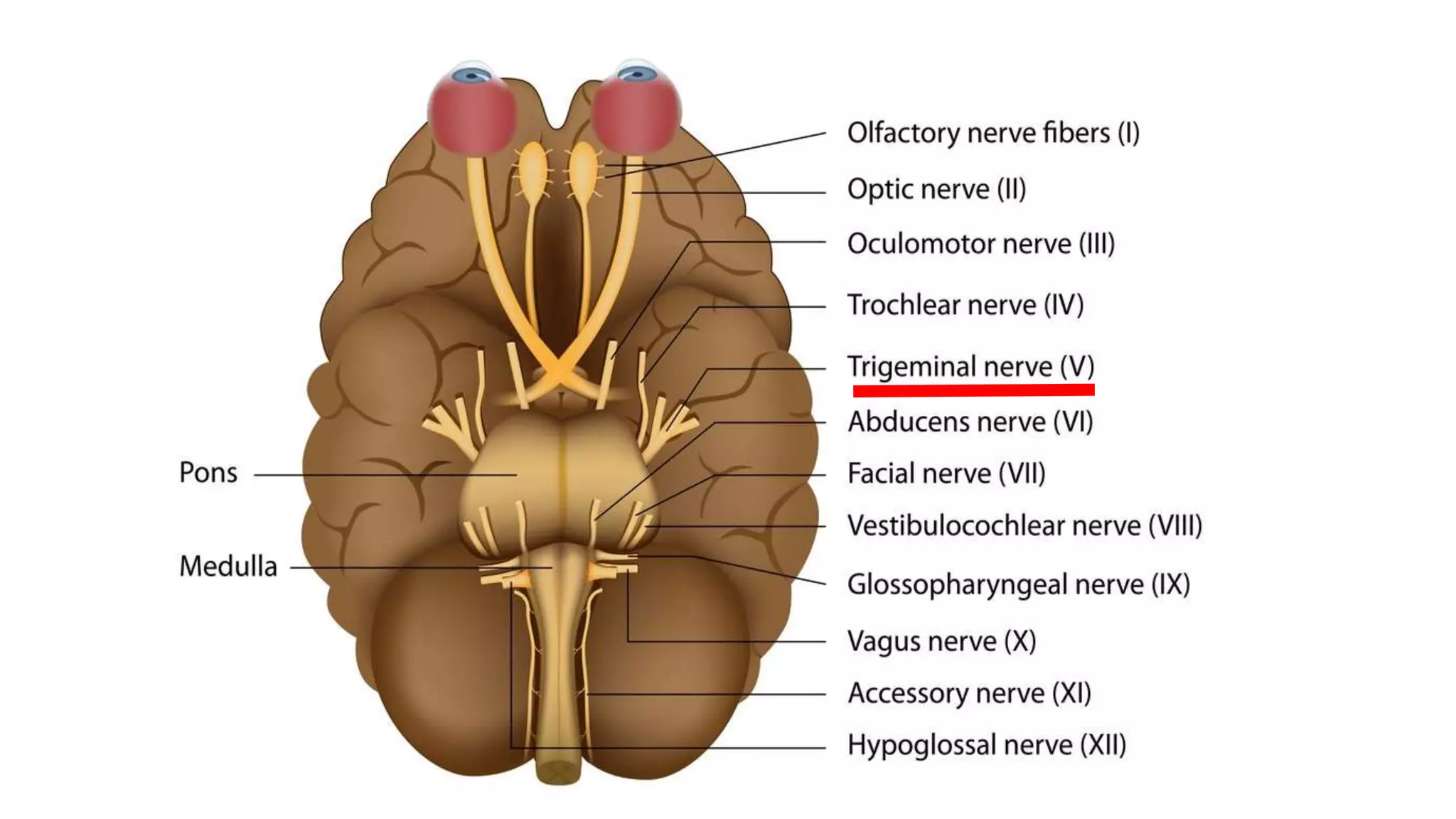
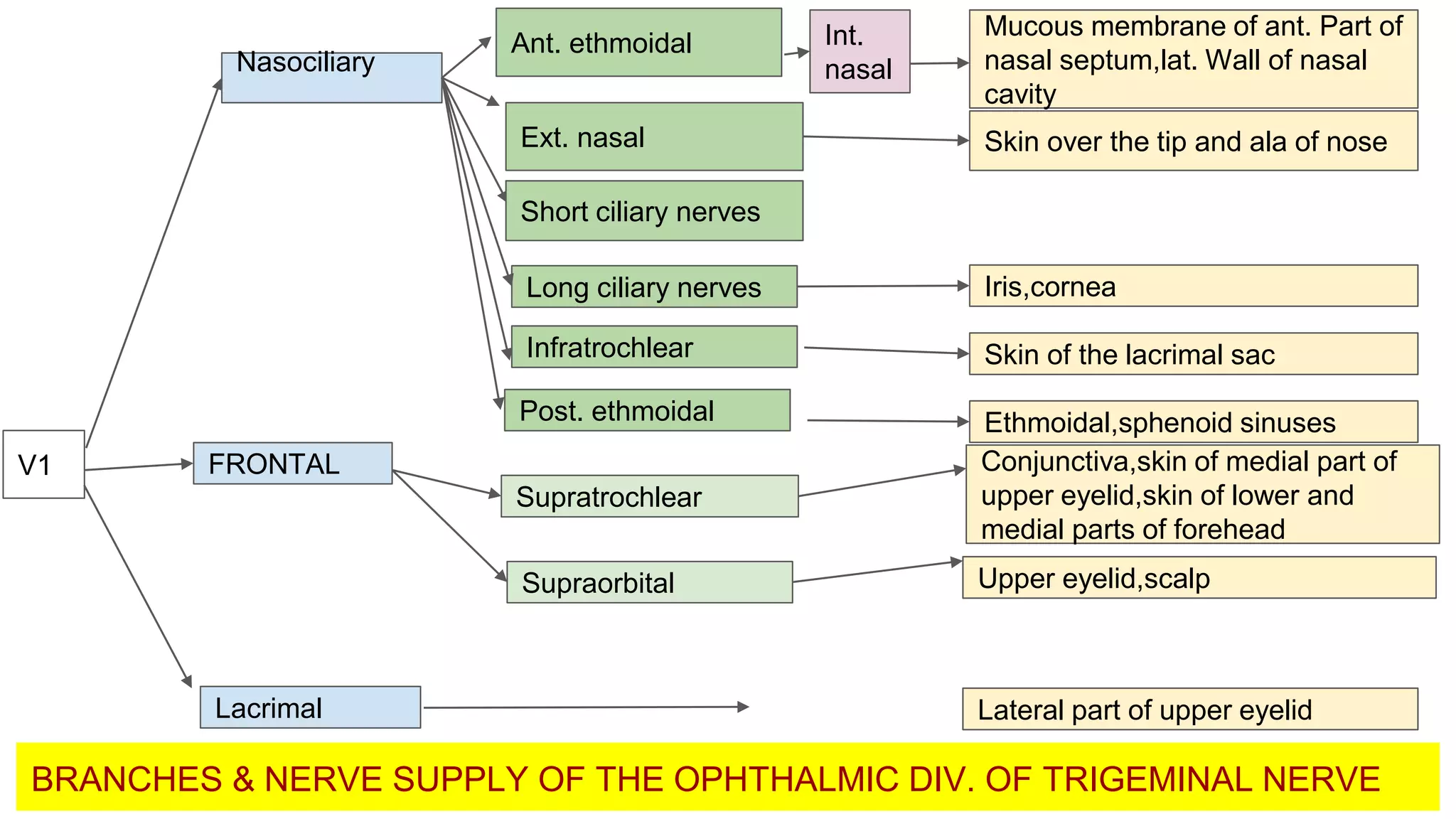
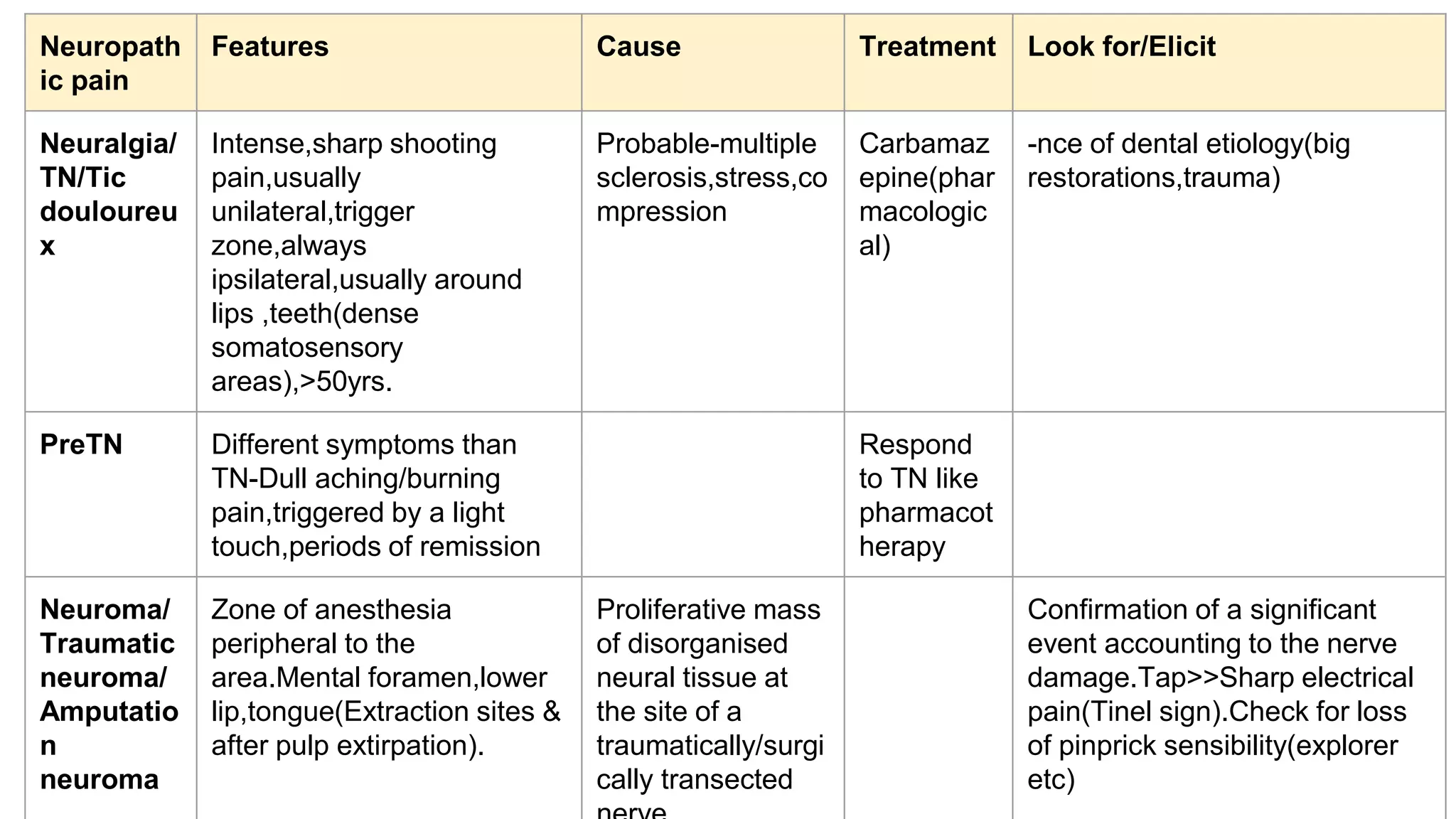
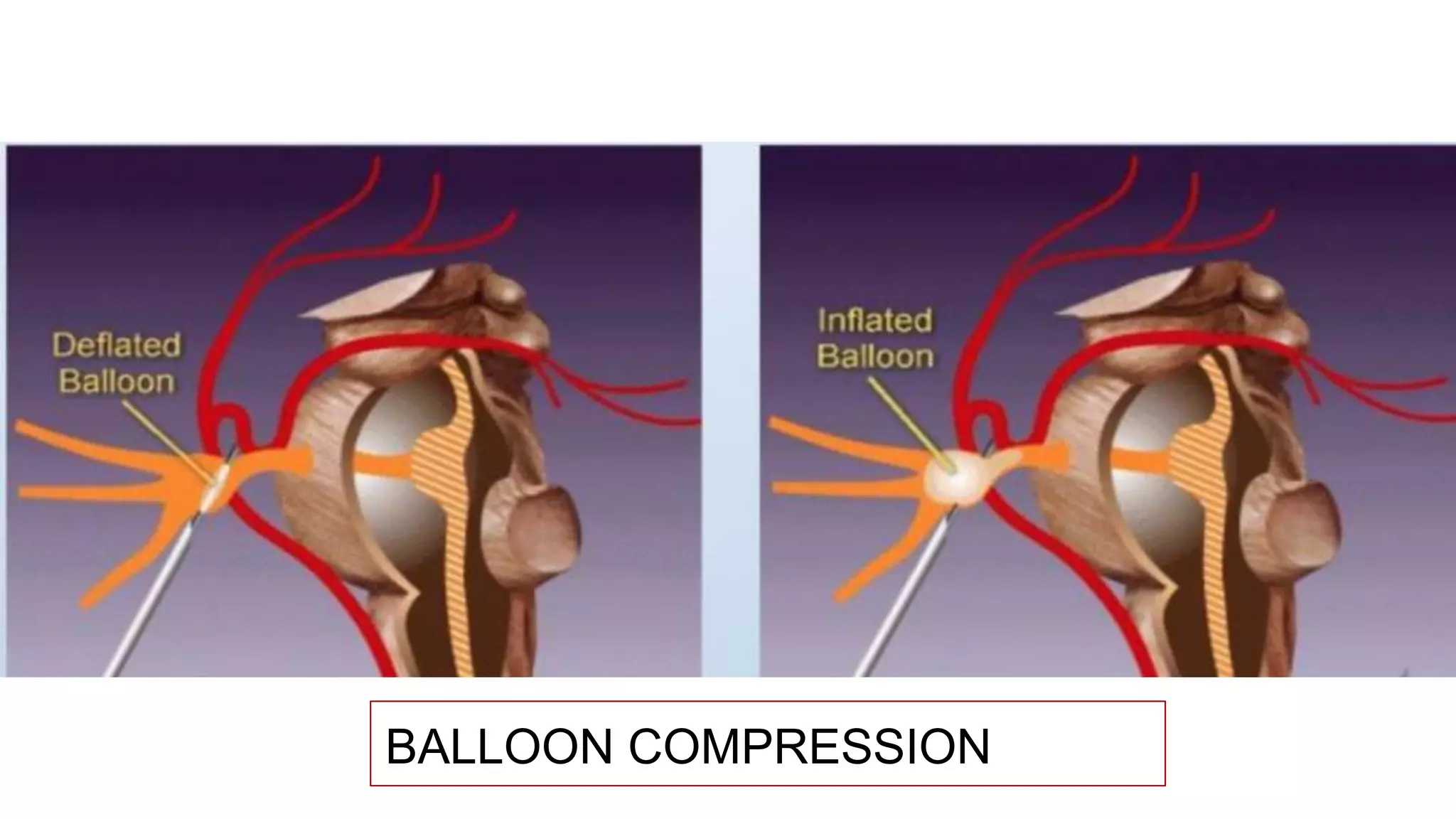
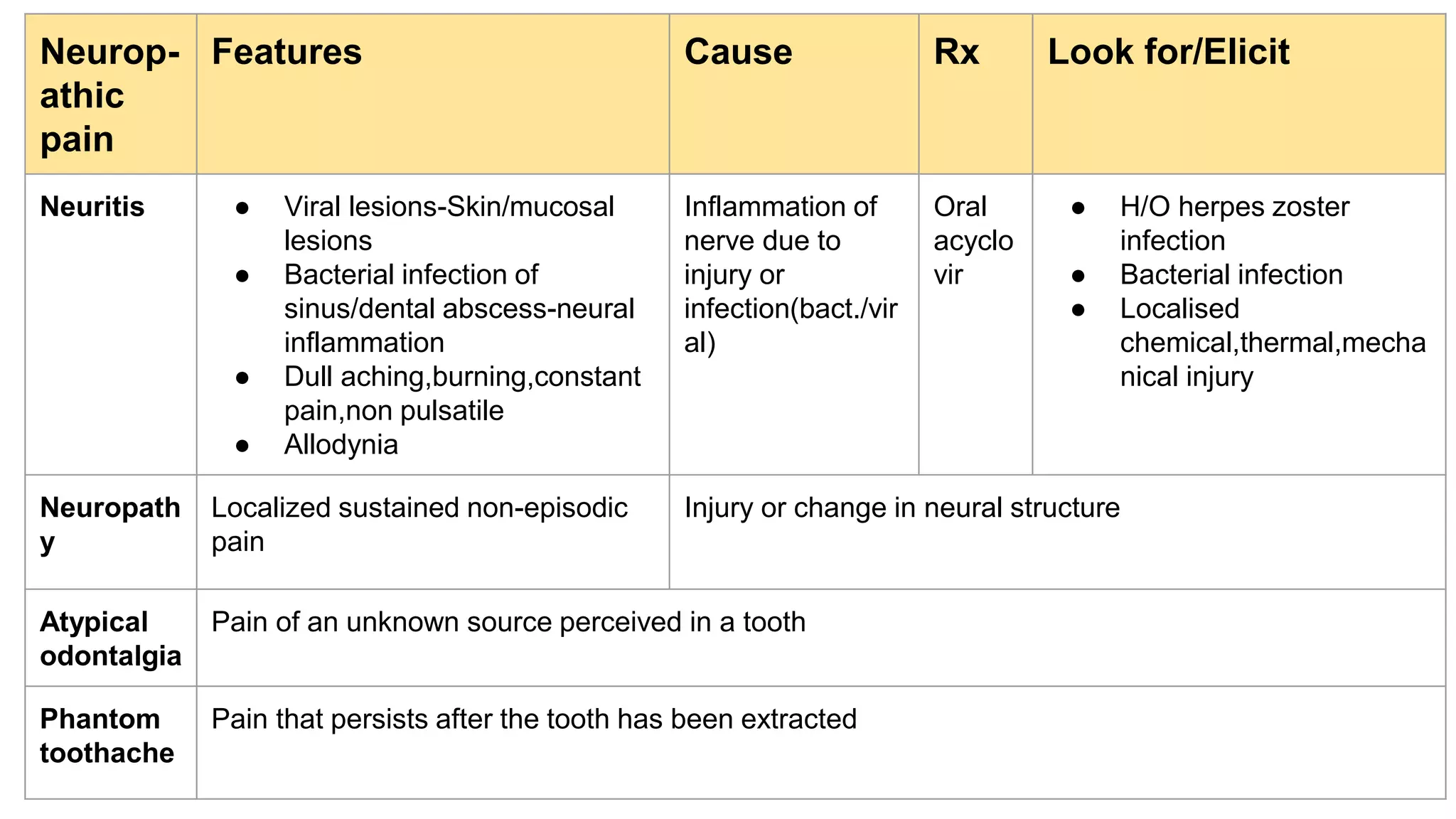
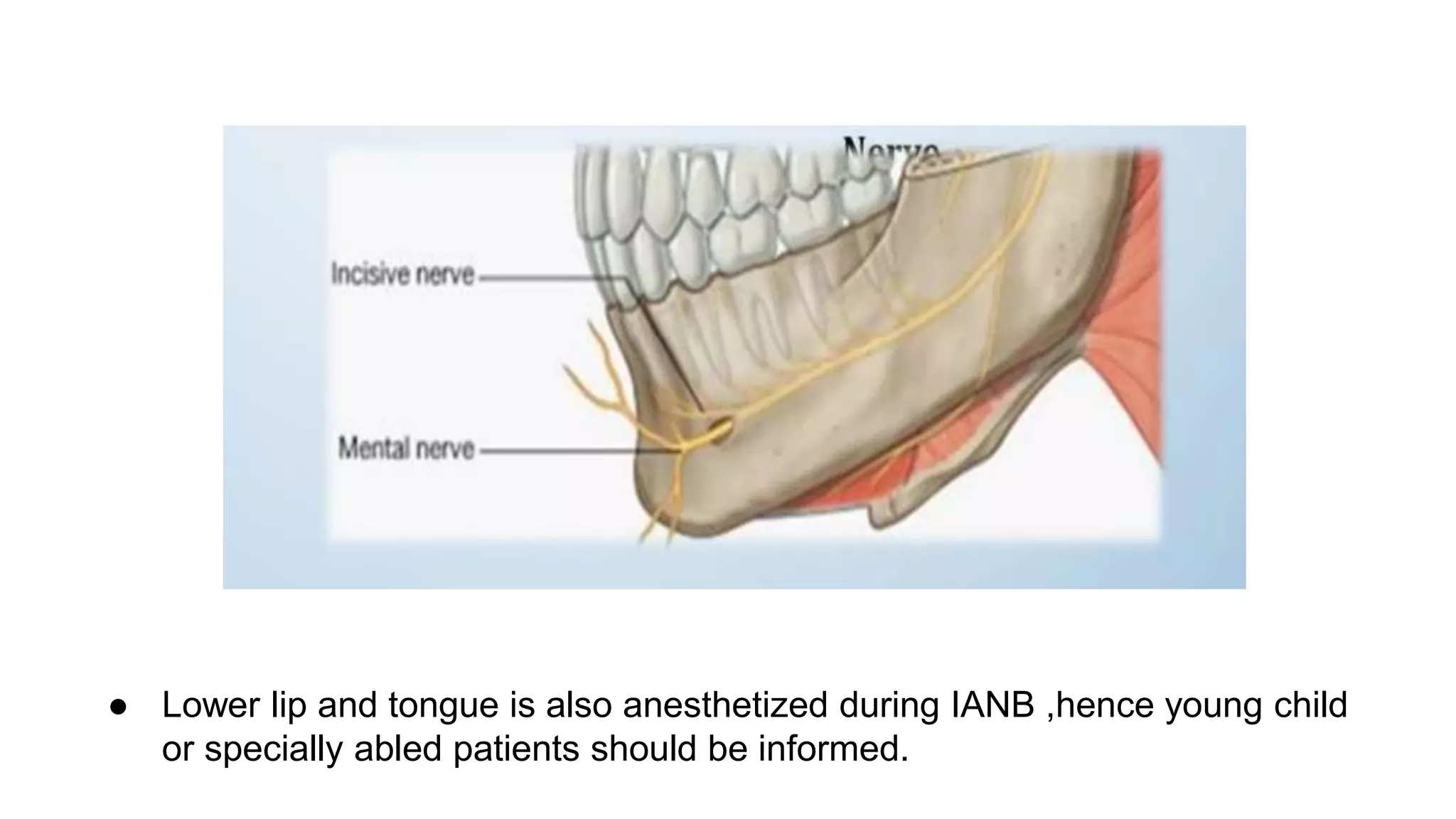
This document provides an overview of the trigeminal nerve (TN) including its anatomy and branches. It discusses the three main divisions of the TN - the ophthalmic, maxillary, and mandibular nerves. For each division, it describes the branches and their nerve supply/sensory distribution. It also discusses applied anatomy concepts in local anesthesia administration and different types of neuropathic pain such as neuralgia, neuroma, neuritis, and neuropathy. Surgical and non-surgical treatment options for trigeminal neuralgia are briefly mentioned. Overall, the document aims to enhance understanding of TN anatomy and its clinical implications.