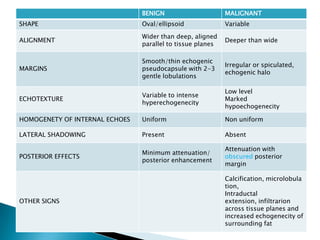
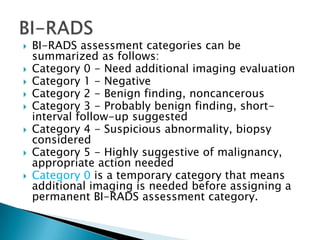
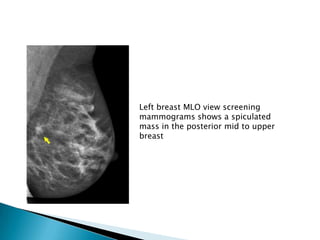
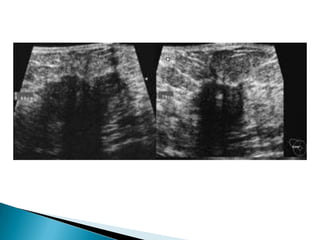
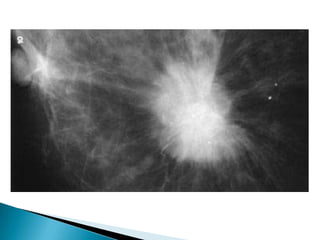
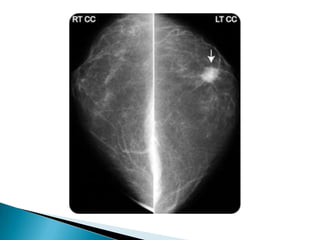
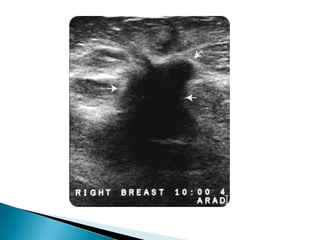
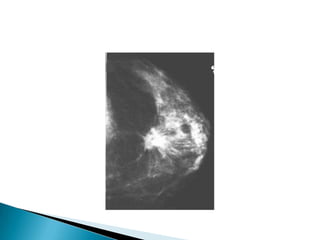
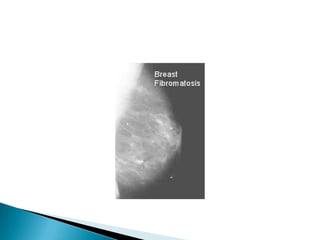
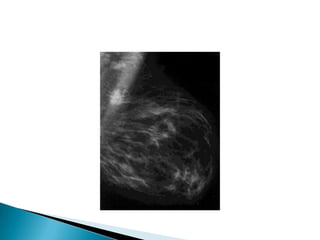
The document discusses how to analyze mammogram images to identify abnormalities. Key steps include assessing quality, comparing left and right images, and systematically searching for masses, calcifications, distortions and other findings. Features of benign and malignant lesions are described, such as shapes of calcifications or margins of masses. Ultrasound may also be used to further evaluate lesions identified on mammogram. Lesions are categorized using BI-RADS assessment to determine if additional imaging or biopsy is needed.