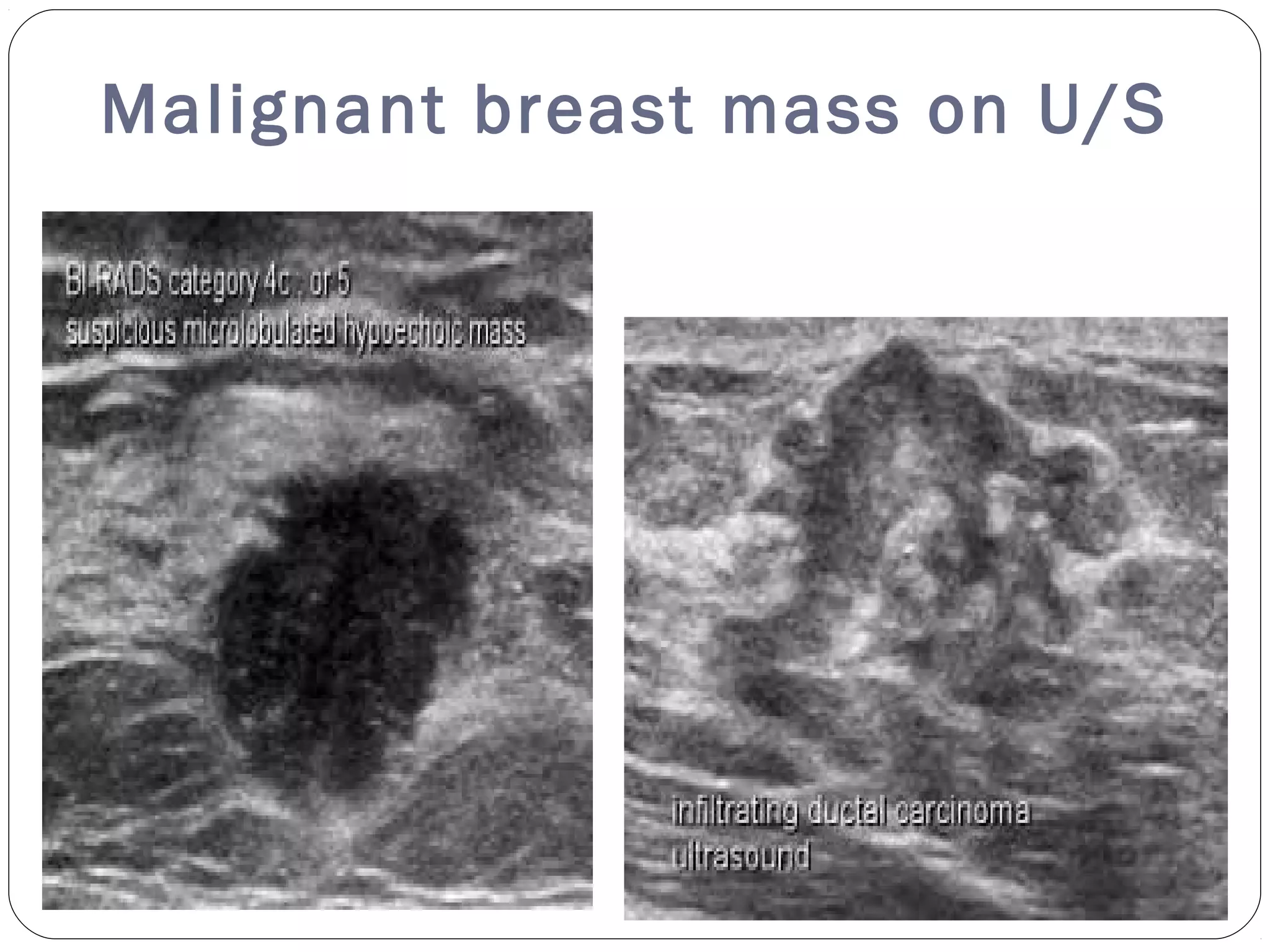
The document discusses the evaluation of breast masses via high-frequency ultrasound, emphasizing its effectiveness in detecting cancers missed by mammography, especially in women with dense breast tissue. It details various types of breast lesions, their ultrasound characteristics, and the classification system for breast imaging, highlighting the significance of techniques like ultrasound elastography in improving diagnostic accuracy. Additionally, it addresses benign and malignant criteria for breast lesions and the value of combined studies for accurate diagnosis.