Downloaded 38 times



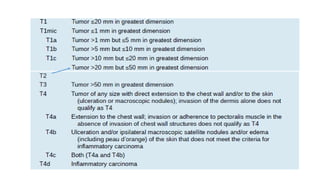
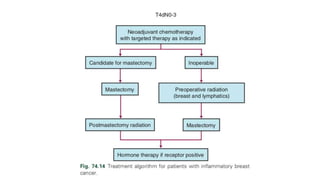
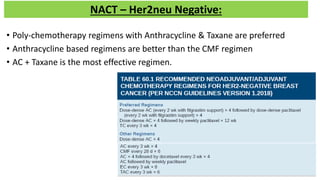
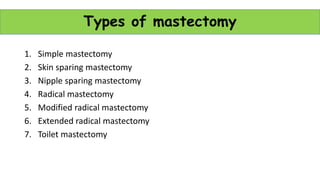
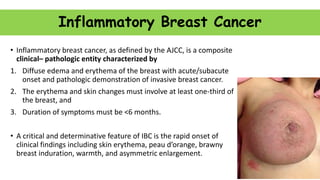
![Benefit with NACT
Trial Randomisation DFS OS Remarks
NSABP B18
[1988-93]
AC adjuvant or
neoadjuvant?
4# AC Sx vs
Sx 4# AC
67% both [5 yr]
58% vs 55% [8 yr]
42 vs 39% [16 yr]
NS
81 vs 80% [5 yr]
72% both [8 yr]
55% both [16 yr]
• Median F/U 16 yrs [2008]
• For OBC
• pCR: significant predictor for
DFS/OS
• BCS rate 68 vs 60% [SS]
• pCR 13%
No DFS/OS benefit with NACT as compared to adjuvant Chemotherapy
Increased rates of BCS
pCR is a significant predictor of DFS/OS
9 yr DFS: 75% [complete responders] vs 58% [partial responders]
9 yr OS: 85% [complete responders] vs 73% [partial responders]](https://image.slidesharecdn.com/locllyadvancedcabreastcopy-210219151048/85/Locally-advanced-ca-breast-LABC-36-320.jpg)
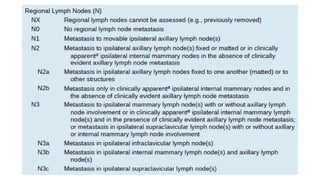
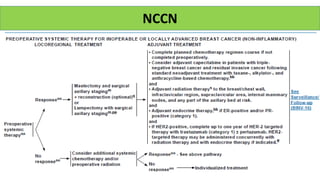
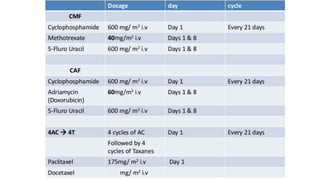
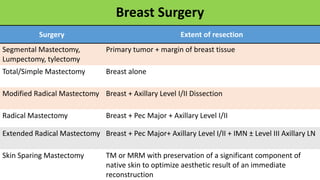
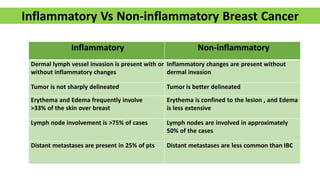
![Breast Conservation: The TMH Experience
• January 1998 to June 2009
• n= 1402 , age 23–76 years, 47.9% postmenopausal
• 63% ER -ve, 62.5% PgR -ve, 20% CerbB2 positive
• Anthracycline-based chemotherapy
• Taxanes given upfront [5%], CMF [1.5%]
• Response: 79.2%
• pCR: 8%
• BCS Rate: 30.4%
• Factors predicting pCR
• Non expression of ER/PR [HR 5.37]
• Presence of LVE [HR 0.25]
• Younger age [HR 1.04]
• Absence of skin involvement [HR 2.05]
• Local Relapse rate: 8% at 30 m](https://image.slidesharecdn.com/locllyadvancedcabreastcopy-210219151048/85/Locally-advanced-ca-breast-LABC-40-320.jpg)
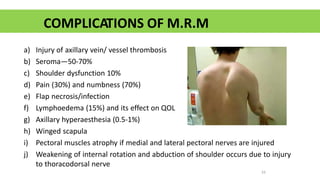
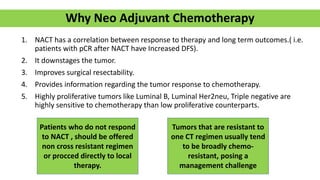
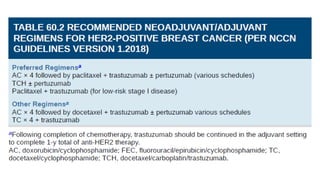
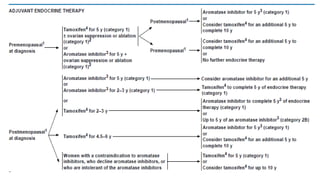
![Adjuvant CT
NSABP-B-01 Scandinavian trial NSABP-B-07
Bonnadonna et al [NEJM 1995]
• 386 N= pts
• Survival benefit with CMF](https://image.slidesharecdn.com/locllyadvancedcabreastcopy-210219151048/85/Locally-advanced-ca-breast-LABC-49-320.jpg)


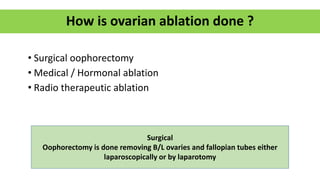
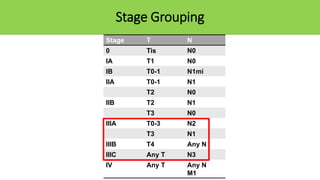
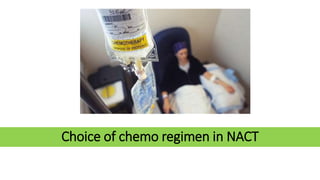
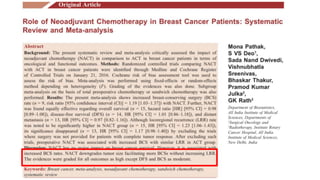
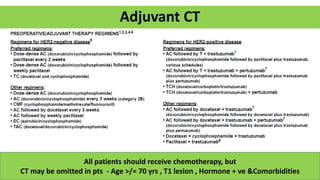
![Oncotype DX
• 21 Gene RT-PCR Assay [recurrence score]
• Indicated only in Early Ca Breast
1. ER/PR +ve tumors
2. Her2neu –ve tumors
3. Stage I Tumors
4. Node –ve
Group Score Treatment
Low Recurrence Group < 18 Only Adjuvant Hormone Therapy, NO CT
Intermediate Recurrence
Group
18 - 30 Only Adjuvant Hormone Therapy or
Adjuvant HT + CT
High Recurrence Group >/= 30 Both Adjuvant CT + HT
It is both Prognostic
and Predictive marker
Done on a tissue
specimen](https://image.slidesharecdn.com/locllyadvancedcabreastcopy-210219151048/85/Locally-advanced-ca-breast-LABC-69-320.jpg)
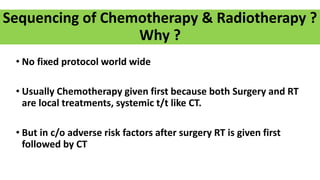


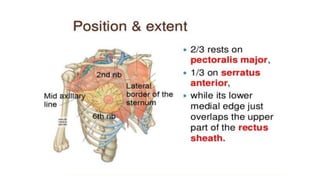
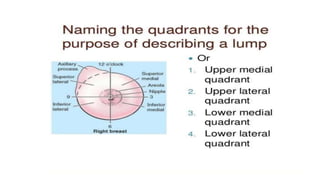
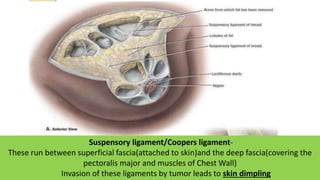
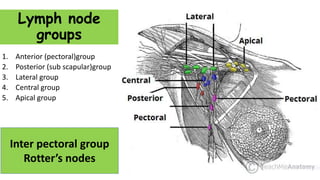
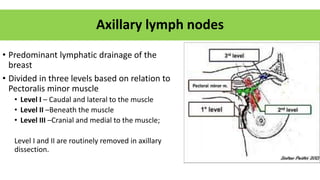
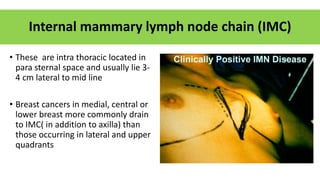
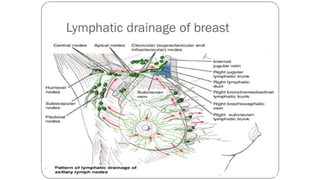
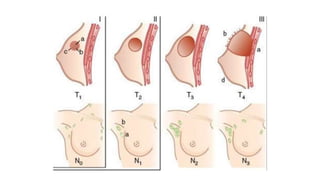
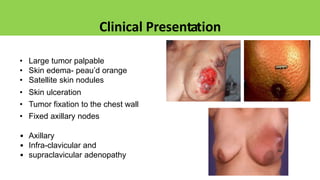
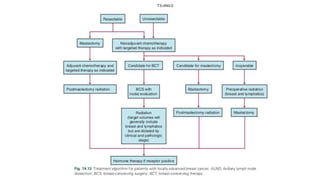
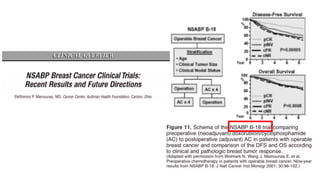
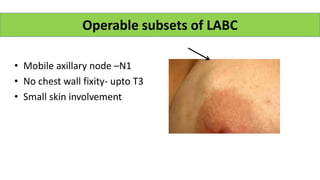
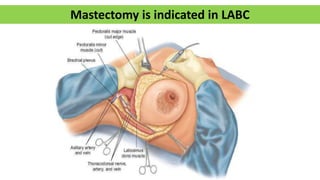
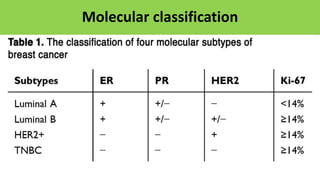
Locally advanced breast cancer is stage III breast cancer characterized by large primary tumors with involved lymph nodes. Key points: - Suspensory ligaments can become invaded, leading to skin dimpling. Lymph nodes are divided into groups for staging. - Axillary nodes are the primary drainage site and are divided into levels based on relation to pectoralis minor muscle. - Internal mammary nodes also commonly involved with medial/central/lower tumors. - Locally advanced breast cancer is usually treated with neoadjuvant chemotherapy to downstage the tumor, followed by surgery and radiation. Molecular subtyping aids treatment planning.













































































