Downloaded 655 times


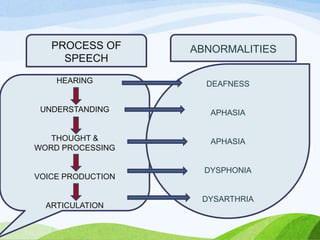
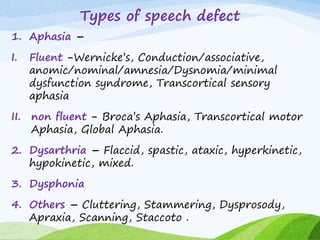
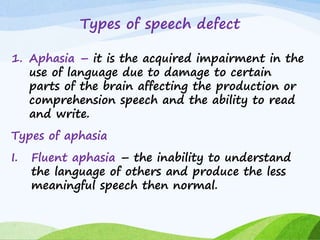
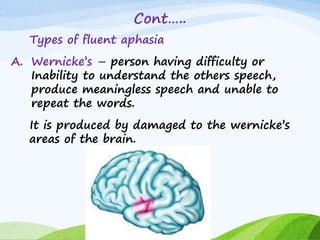







Speech defect is a type of communication disorder that disrupts normal speech. Speech therapy is a rehabilitative procedure to help people with communication or swallowing problems. Speech defects are classified based on the sounds a patient can produce, whether sounds need demonstration to be stimulated, and sounds that cannot be produced. Major types include aphasia, dysarthria, dysphonia, cluttering, stammering, and apraxia. Diagnostic evaluations include history, physical exams of the head and neck, and tests like laryngoscopy. Management involves correcting underlying conditions, special education, and speech therapy techniques like remediation, language exercises, and swallowing therapy.















































































