Downloaded 308 times




















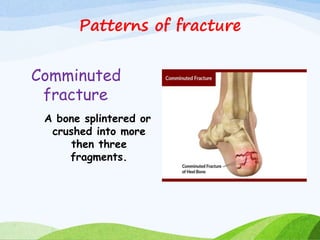






















































This document provides information on fractures, including definitions, types, patterns, causes, clinical manifestations, diagnostic evaluation, management, and nursing care. It defines a fracture as a break in the continuity of bone. The objectives are to introduce fractures, explain causes such as direct blows or muscle contractions, and describe types including complete, incomplete, closed and open. Patterns like transverse, oblique, and comminuted are also outlined. Clinical signs involve pain, swelling and deformity. Management includes reduction, immobilization with casting or fixation devices, and exercises. Complications can be early like fat embolism or delayed like nonunion. Nursing care focuses on pain management, range of motion, hygiene, nutrition, and mobility assistance














































































