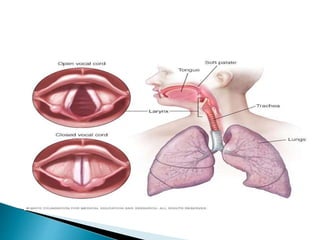
Speech is the vocalized form of human communication that involves articulation using the mouth, voice produced by vocal cords, and fluency or rhythm of speech. Speech production requires respiration from the lungs, phonation by the vocal cords, and articulation using structures in the mouth and nose. Hoarseness or roughness of voice can be caused by issues with the vocal cords such as paralysis, tumors, or nodules that prevent normal vibration. Various types of dysphonia including adductor, abductor, and mixed can be diagnosed and treated through laryngoscopy, botulinum toxin injections, voice therapy, and other methods.































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

















