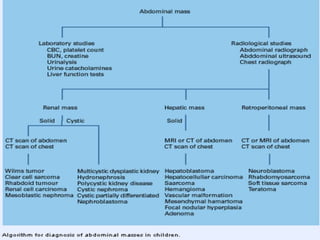
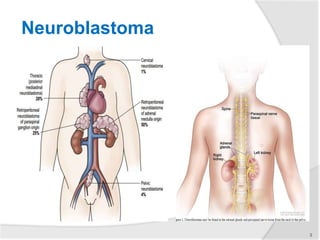
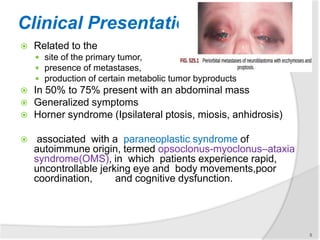
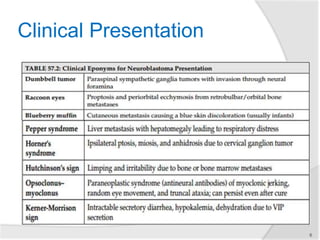
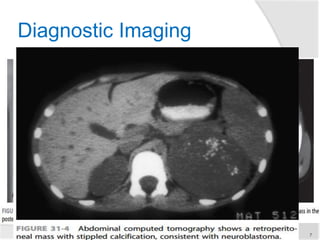
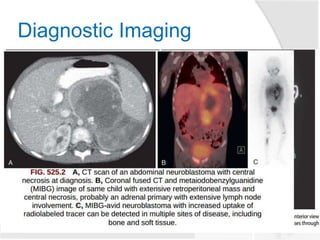
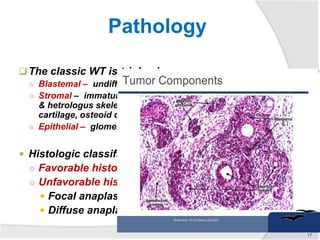
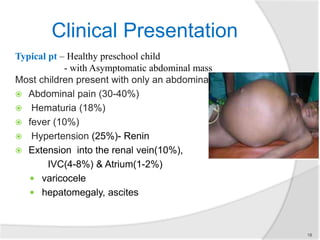
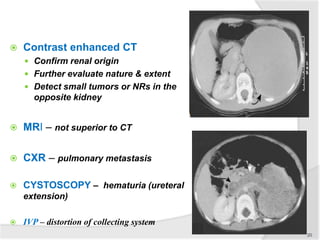
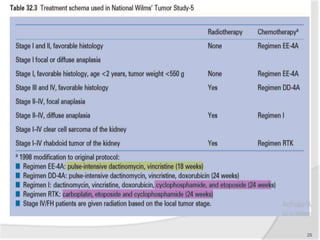
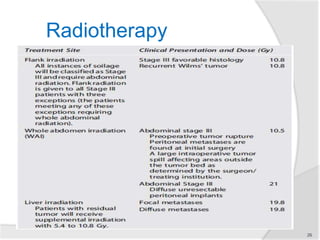
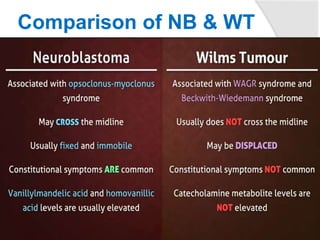
This document provides information on neuroblastoma and Wilms' tumor, two common pediatric abdominal masses. Neuroblastoma arises from neural crest tissue and is the most common extracranial solid tumor in children. It typically presents as an abdominal mass and can metastasize. Treatment involves chemotherapy, surgery, and sometimes stem cell transplant depending on risk factors. Wilms' tumor arises from the kidneys and is also typically detected as an asymptomatic abdominal mass in young children. Staging involves evaluating the extent of the primary tumor and presence of metastases to determine the appropriate treatment, which usually involves surgery and chemotherapy. Both tumors require a multidisciplinary approach including imaging, biopsy, surgery, and chemotherapy.