Download to read offline

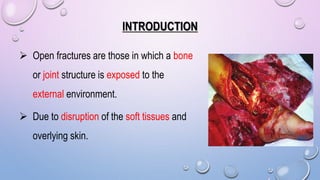





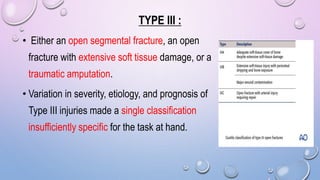
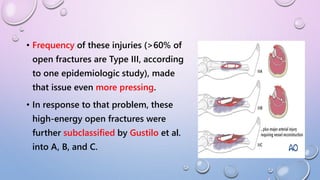



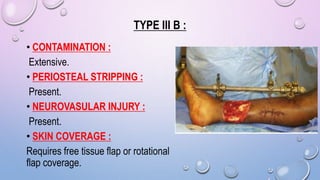


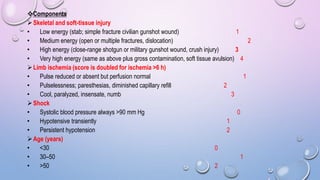

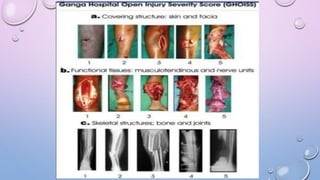




This document discusses the classification of open fractures. It begins with a brief history, noting that open fractures were first recognized by Egyptians and Hippocrates advocated debridement. It then details several classification systems for open fractures. The most widely used system is the Gustilo-Anderson classification, which considers wound size, soft tissue damage, and contamination. Type III fractures are further divided into subclasses A, B, and C based on severity. Other classification systems discussed include MESS, GHOISS, and Oestern and Tschernes. Complications of open fractures include shock, compartment syndrome, and infection.






























![[TRAUMATOLOGY] SOFT TISSUE MANAGEMENT AND RECONSTRUCTION IN ORTHOPAEDICS EMER...](https://cdn.slidesharecdn.com/ss_thumbnails/softtissuemanagementandreconstraction-210729080619-thumbnail.jpg?width=640&height=640&fit=bounds)













![SOFT TISSUE INJURY [Recovered].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/classificationofsofttissueinjuryrecovered-220424142623-thumbnail.jpg?width=640&height=640&fit=bounds)










![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











