
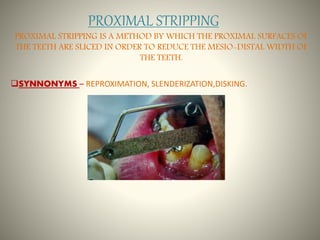

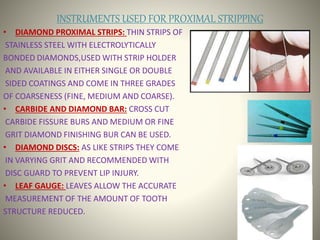
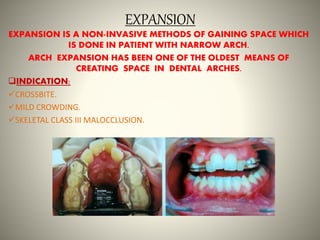

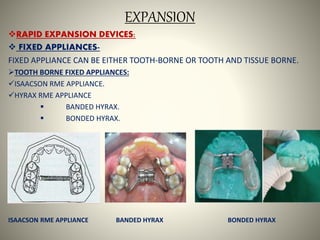
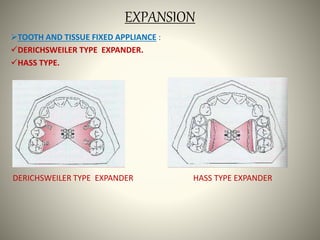


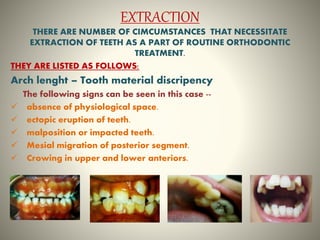



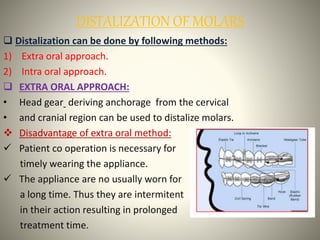
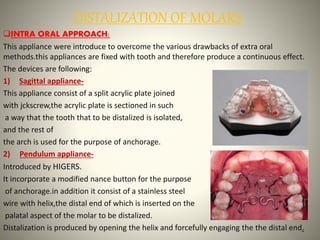
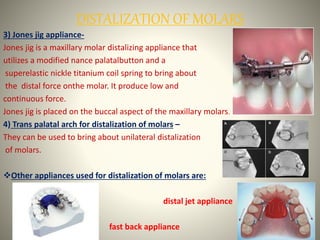
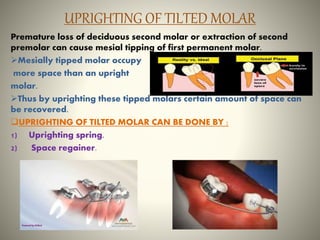
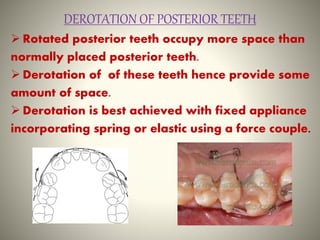



This document discusses various methods for gaining space in orthodontic treatment, including proximal stripping, arch expansion, extraction, distalization of molars, uprighting tilted molars, derotation of posterior teeth, and proclination/flaring of anterior teeth. It provides details on techniques such as rapid maxillary expansion using devices like Hyrax or bonded expanders, extraction of first premolars, and distalization of molars using appliances like pendulum or Jones Jig. The document also covers indications, advantages, and disadvantages of different space gaining methods.






























































































