Download to read offline


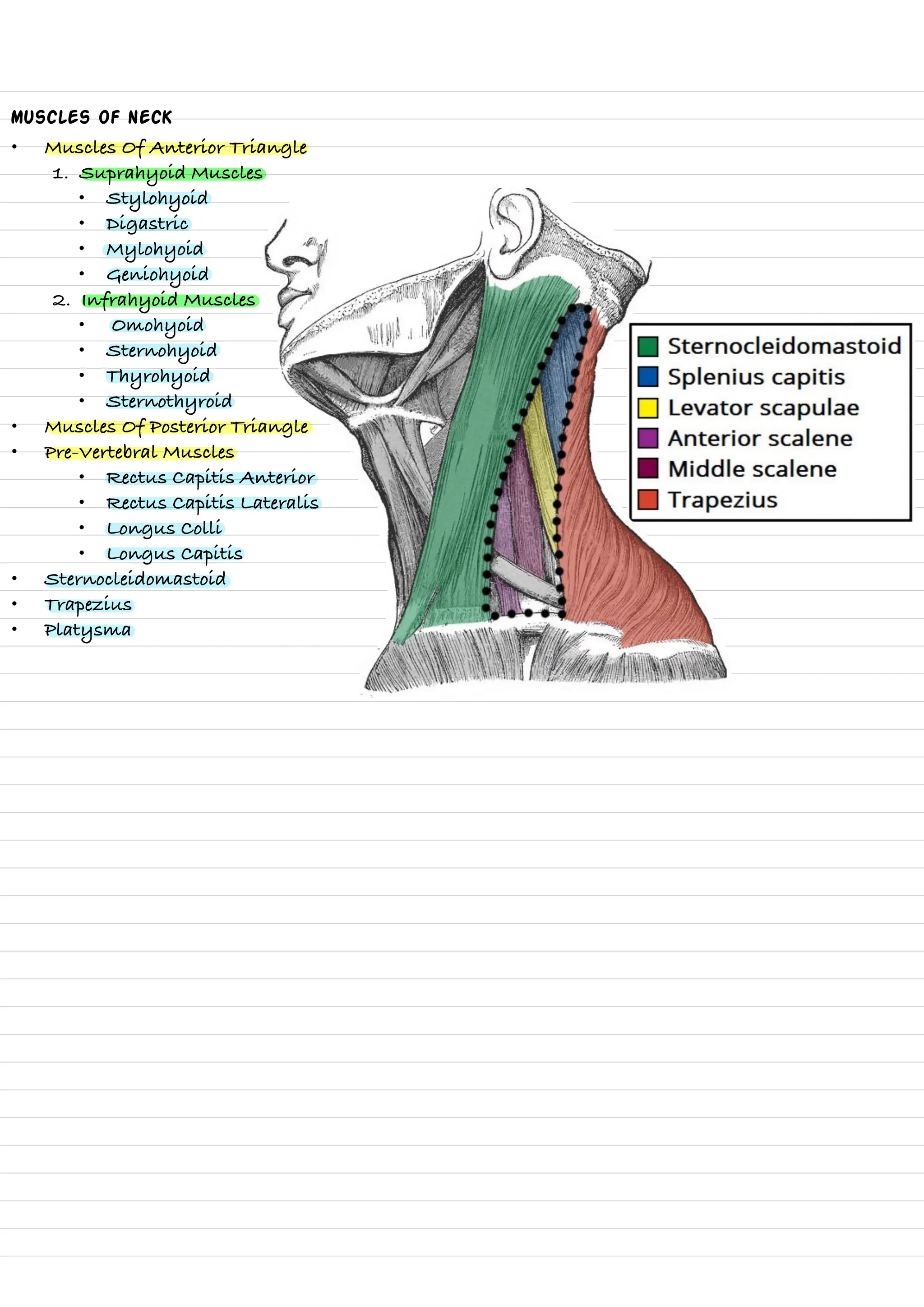
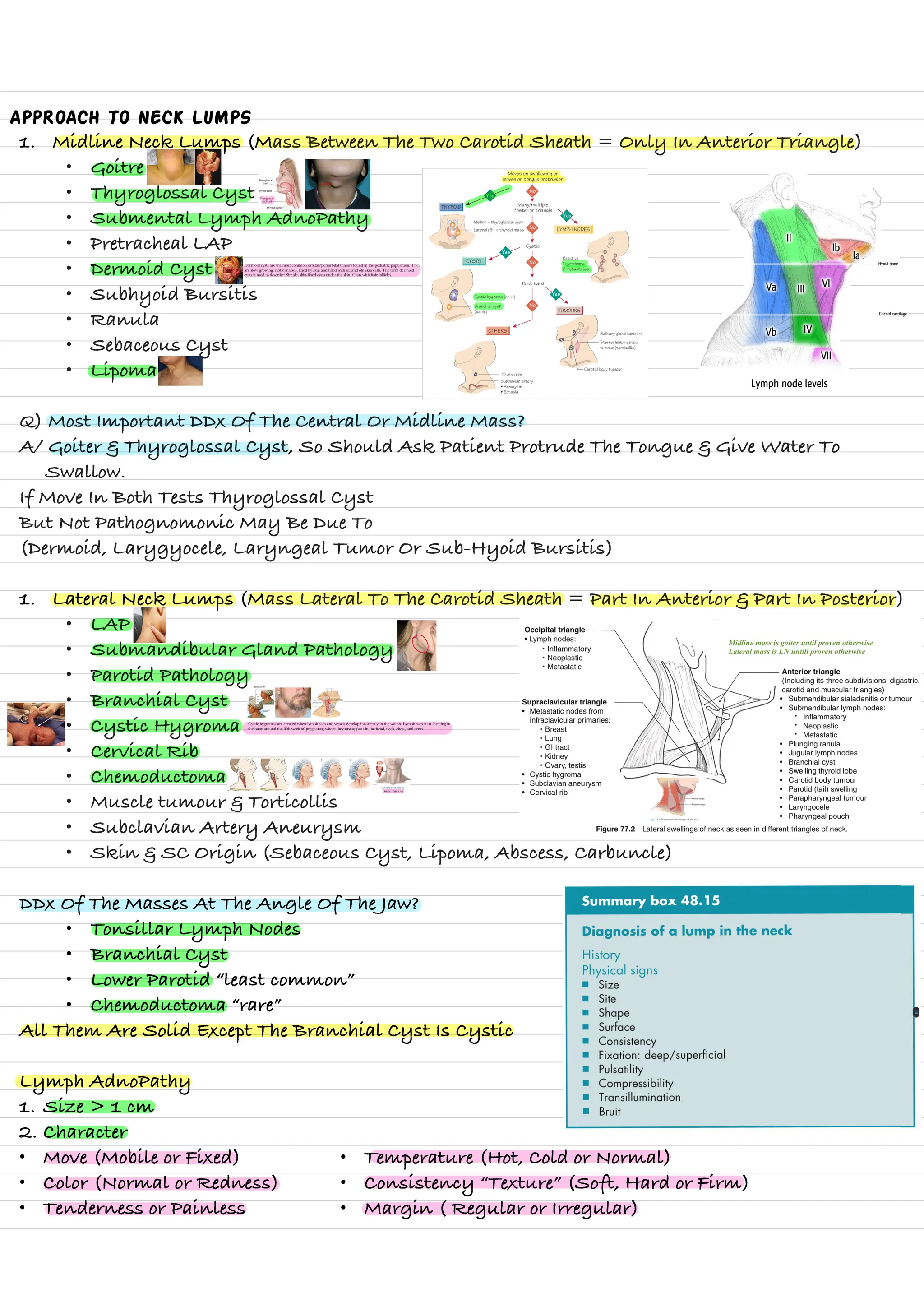












**Overview of Neck Lumps and Surgical Anatomy** • **Key Focus Areas**: * **Surgical Anatomy of the Neck** - Detailed breakdown of neck compartments - Anatomical structures and layers - Muscle groups and triangles * **Neck Lump Classification** - **Types of Neck Lumps**: - Midline neck lumps - Lateral neck lumps - Congenital anomalies - Inflammatory conditions - Tumors * **Diagnostic Approach** - **Comprehensive Examination Techniques** - Clinical assessment - Laboratory investigations - Imaging studies - Biopsy methods * **Specific Conditions Covered** - Thyroid diseases - Lymphadenopathy - Cystic hygromas - Branchial cysts - Parathyroid disorders • **Primary Medical Disciplines**: * **Surgical Anatomy** * **Endocrinology** * **Oncology** * **Diagnostic Medicine