Small bowel obstruction and Intestinal Fistulas
•Download as PPTX, PDF•
15 likes•4,558 views

Small bowel obstruction is a common surgical condition where the small intestine becomes blocked. The most frequent cause is adhesions from prior abdominal surgery, accounting for up to 75% of cases. Symptoms include abdominal pain, nausea, vomiting and constipation. Diagnosis involves imaging like abdominal x-rays showing dilated bowel loops or CT scans identifying transition points. Treatment depends on the severity and cause but generally involves surgery to remove blockages or adhesions and repair hernias or tumors. Outcomes are good if caught early but mortality rises with delay in surgery or if the obstruction becomes strangulated.

More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Small bowel obstruction and Intestinal Fistulas
Similar to Small bowel obstruction and Intestinal Fistulas (20)
More from Jose Cortes
More from Jose Cortes (8)
Recently uploaded
Recently uploaded (20)
Small bowel obstruction and Intestinal Fistulas
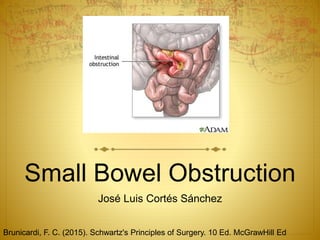
- 1. Small Bowel Obstruction José Luis Cortés Sánchez Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed
- 2. Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed Epidemiology Most frequently encountered surgical disorder of the small intestine Anatomic relationship to intestinal wall: 1.- Intraluminal: 2.- Intramural 3.- Extrinsic
- 3. Intraabdominal adhesions related to prior abdominal surgery account for up to 75% of cases 300,000 patients are estimated to undergo surgery to treat them annually From 1988 to 2007 there was no decrease in this rate Ongoing problems with this “old” disease Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed
- 4. Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed Other causes: Hernias, malignant, Chron’s Few are due to primary bowel tumors
- 5. Congenital usually become evident during childhood, but sometimes are not i.e. Intestinal malrotation, mid-gut volvolus (without history) Superior mesentric artery Sx. (rare etiology) Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed
- 6. Pathophysiology Gas and fluid acumulate Intestinal activity increases Pain and diarrhea Swallowed air and produced Swallowed liquids and GI secretions Bowel distends IM/ IL pressure rises Motility is eventually reduced Luminal flora changes If IM pressure high enough perfusion is impaired ischemia - necrosis Strangulated bowel obstruction Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed
- 7. Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed Partial Allows passage of some fluid and gas Event progression occur more slowly Less likely to become strangulated Closed-loop Particularly dangerous E.g. volvolus Rapid rise in luminal pressure Rapid progression to strangulation
- 8. Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed Clinical presentation Colicky abdominal pain, nausea, vomiting, obstipation More vomiting w/proximal than distal Feculent? bacterial overgrowth (more established) Continuos passage of flattus/stool >6-12 hours= Partial
- 9. Signs Abdominal distention (more if distal) Initially hyperactive bowel sounds then minimal Lab: Intravascular volume depletion Hemoconcentration Electrolyte abnormalities Mild leukocytosis Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed
- 10. Strangulated Abd. pain disproportionate to degree of abd findings -suggestive of intestinal ischemia Tachycardia, Localized abd tenderness Fever Marked leukocytosis Acidosis Alert! Prompt early surgical intervention! Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed
- 11. Diagnosis 1.-Distinguishing mechanical obstruction from ileus 2.-Determine the etiology 3.-Discriminate partial from complete 4.-Discriminate simple from strangulated Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed
- 12. History Prior abd operations Abd disorders (cancer, IBD) Meticulous search for hernias(inguinal, femoral) Dx.- confirmed by radiographic exams Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed
- 13. Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed Abdominal series Rx of the abdomen patient in supine Abdomen w/patient upright Rx of the chest w/patient in upright Most specific triad: -Dilated small bowel loops (>3 cm in diameter) -Air-fluid levels on upright -Paucity of air in colon S= 70-80% E= lowDDX.- Ileus, colonic obstruction FN= proximal; fluid but no gas Closed-loop Despite these limitations, abdominal radiographs remain an important study in patients with suspected small bowel obstruction because of their wide- spread availability and low cost
- 14. Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed CT scan Discrete transition zonew/dilation of proximal Decompression of distally Contrast that doesn’t pass beyond transition Colon with little gas or fluid S= 80-90% E= 70-90% -CT may also provide evidence of closed- loop/strangulation - -Closed-loop U-/C- shaped bowel+ radial messenteric vessels in torsion point -Strangulation Thickening of bowel wall, pneumatosis intestinalis, portal venous gas, mesenteric haziness Poor uptake of IV contrast CT also reveals the etiology
- 15. Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed Appearance of contrast in colon w(24hrs) is predictive of non- surgical resolution Reduce overall length of hospitalization S= 50% , for low-grade or partial Small bowel series/ Enteroclysis can be helpful
- 16. Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed Therapy Marked depletion of IV volume –> fluid resuscitation is integral to treatment Central venous o pulmonary artery catheter assist fluid management (CVS or severe) Antibiotics? No data to support it Isotonic fluid IV + Bladder catheter NG tube to evacuate stomach. Not jejunum nor ileum Decreases nausea, vomiting, distention, aspiration
- 17. “the sun should never rise and set on a complete bowel obstruction.” Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed
- 18. Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed nonoperative aproaches R/O closed-loop ; neither intestinal ischemia Observe closely and undergo serial exams Early surgical intervention Minimize the risk for strangulation Morbimortality Signs and lab tests and imaging don’t distinct between them Goal? operate before onset of ischemia A period of observation and NG decompression, provided no tachycardia, tenderness or WBC increases
- 19. Conservative therapy 1. Partial small bowel obstruction 2. Obstruction occurring in the early postoperative 3. Intestinal obstruction due to Crohn’s disease 4. Carcinomatosis Strangulation is unlikely to occur. Succesful in 65-81% Of these 5-15% don’t improve at 48 hrs Patients with partial obstruction thath do not improve at 48h should undergo surgery!0 -Occur in 0.7% patients undergoing laparotomy. -Pelvic surgery, especially colorectal procedures, have the greatest risk. -Should be considered if -symptoms of intestinal obstruction occur after the initial return -Function fails to return within the expected 3 to 5 days after -25-33% of patients with -Even in cases in which the obstruction is related to recurrent malignancy, palliative resection or bypass can be performed. -Patients with obvious carcinomatosis pose a difficult challenge, given their limited prognosis. May be best achieved by a bypass procedure Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed
- 20. Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed Adhesions lysed Tumors resected Hernias reduced and repaired. The affected intestine should be examined, and nonviable bowel resected. If the patient is hemodynamically stable, short lengths of bowel of questionable viability should be resected Bowel of uncertain viability should be left intact and the patient re-explored in 24 to 48 hours in a “second- look” operation. Criteria suggesting viability: -normal color, -peristalsis, -marginal arterial pulsation Operative procedure varies according to the etiology Laparascopic procedure have a quicker recovery, less complications, and lower costs. Distended loops of bowel can interfere with adequate visualization, early cases likely due to a single adhesion Conversion rate to open surgery is between 17% and 33%
- 21. Outcomes Prognosis is related to the etiology Less than 20% of conservative patients will have a readmission over the subsequent 5 years The perioperative mortality rate associated with surgery for nonstrangulating small bowel obstruction is less than 5%, Mortality rates associated with surgery for strangulating obstruction range from 8% to 25%. Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed
- 22. Brunicardi, F. C. (2015). Schwartz's Principles of Surgery. 10 Ed. McGrawHill Ed Prevention Good surgical technique, careful handling of tissue, and minimal use and exposure of peritoneum to foreign bodies form the cornerstone of adhesion prevention. Colorectal or pelvic surgery, hospital readmission rates of greater than 30% over the subsequent 10 years . Seprafilm
- 25. fistula abnormal communication between two epithelialized surfaces. internal fistula .- between two parts of the GI tract or adjacent organs external fistula involves the skin or another external surface epithelium. Over 80% of enterocutaneous fistulas represent iatrogenic complications that occur as the result of enterotomies or intestinal anastomotic dehiscences. Spontaneously without antecedent iatrogenic injury are Crohn’s disease or cancer. low-output fistulas Entero- cutaneous fistulas that drain less than 200 mL of fluid per day high-output fistulas. those that drain more than 500 mL of fluid per day
- 26. Pathophysiology Low-resistance enteroenteric bypass malabsorption Enterovesicular Recurrent UTI’s Drainage from enterocutaneous irritates skin excoriation Loss of enteric luminal contents (high-output) dehydration, electrolyte abnormalities, malnutrition
- 27. Fistulas have the potential to close spontaneously, but:
- 28. Clinical Presentation Fever Leukocytosis prolonged ileus abdominal tenderness, wound infection evident between the 5th-10th postoperative days. initialsigns. Iatrogenic enterocutaneous fistulas The diagnosis is obvious when drainage of enteric material occurs. These fistulas are often associated with
- 29. Diagnosis CT scanning following the administration of enteral contrast Most useful initial test? Leakage of contrast material from the intestinal lumen can be observed. Intraabdominal abscesses should be sought and drained percutaneously. -Small bowel series or enteroclysis examination can be obtained to demonstrate the fistula’s site of origin in the bowel. -Useful to R/O the presence of intestinal obstruction distal to the site of origin. If the anatomy of the fistula is not clear on CT scanning? A fistulogram,
- 30. Therapy 1. Stabilization. Fluid and electrolyte resuscitation is begun. Nutrition is provided, usually through the parenteral route initially. Sepsis is controlled with antibiotics and drainage of abscesses. The skin is protected from the fistula effluent with ostomy appliances or fistula drains. 2. Investigation. The anatomy of the fistula is defined 3. Decision. Tx options considered, and timeline for conservative 4. Definitive management. surgical procedure 5. Rehabilitation.
- 31. Objective is to increase the probability of spotaneous closure. Nutrition and time are the key components of this approach. Most patients will require TPN however, a trial of oral enteral nutrition should attempted in patients w low-output fistulas originating from the dis intestine.Octreotide is a useful adjunct, particularly in patients with high-output fistulas; -reduces the volume of fistula output thereby facilitating fluid and electrolyte management.
- 32. Timing of Surgical Intervention. 2 to 3 months of conservative therapy before considering surgical intervention. surgical intervention after this time period is associated with better outcomes and lower morbidity 90% of fistulas that are going to close do so within 5 weeks fails to resolve during this period ? fistula tract, together with the segment of intestine from which it originates, should be resected. Simple closure of the opening in the intestine from which the fistula originates is associated with high recurrence rates.
- 33. Outcomes “FRIEND” Foreign body within the fistula tract Radiation enteritis Infection/Inflammation at the fistula origin Epithelialization of the fistula tract Neoplasm at the fistula origin Distal obstruction of the intestine Over 50% of intestinal fistulas close spontaneously.
- 34. 153 cases of enterocutaneous fistulas Majority were found to originate from the small bowel Patients having undergone 5 or + previous surgeries. 30-day mortality of approximately 4% 1-year mortality of 15%. Morbidity was over 80%. First surgical repair attempt was successful 70% of cases Some patients requiring up to three attempts at surgical repair. Owen RM, Love TP, Perez SD, et al. Definitive surgical treatment of enterocutaneous fistula: outcomes of a 23-year experi- ence. Arch Surg. 2012;15:1.
- 35. A 43-year-old woman comes to the emergency department with a 3-day history of abdominal distention, nausea, and vomiting. She also reports decreased urine output over the last 24 hours. She has a history of total abdominal hysterectomy 5 years ago for benign disease. She does not take any medications. Her pulse is 110 beats/minute. Her abdomen is distended and there is mild diffuse tenderness. Bowel sounds are hyperactive. The rest of her exam is normal. Serum electrolytes are sodium—140, chloride—90, bicarbonate—32, and potassium—4.0. Which of the following is the most appropriate initial intravenous fluid to administer to this patient? A.-D5 1⁄2 normal saline with 40 mEq KCl/L B. Lactated Ringer’s solution C. Normal saline D. Colloidal starch solution E. 5% albumin in normal saline