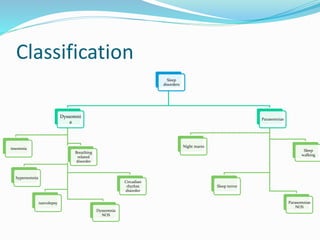
This document provides an overview of sleep, its functions, stages and disorders. It defines sleep as a state of unconsciousness where the brain is more responsive to internal stimuli. Sleep has restorative and homeostatic functions. There are two main stages - NREM and REM sleep. Dyssomnias are disorders of sleep quantity/timing and include insomnia, hypersomnia, narcolepsy and sleep apnea. Parasomnias involve abnormal behaviors during sleep transitions and include nightmares, sleepwalking and REM sleep behavior disorder. Many common sleep disorders are described along with their symptoms, causes and treatment options.
































![Sleep disorders [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/sleepdisordersautosaved-180531135608-thumbnail.jpg?width=640&height=640&fit=bounds)







































