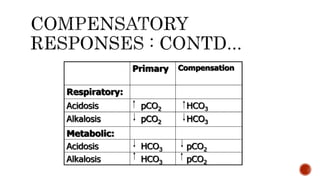
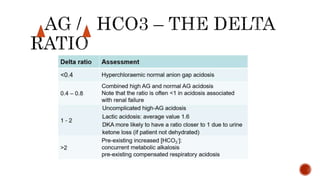
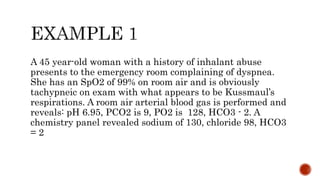
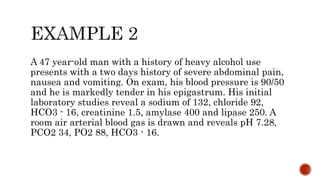
The document presents an overview of acid-base disorders, outlining key concepts such as acidosis, alkalosis, and their metabolic and respiratory types. It includes diagnostic considerations, compensation mechanisms, and clinical case examples illustrating various acid-base imbalances and their management. Treatment focuses on addressing underlying causes while considering both acute and chronic changes in acid-base status.






















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















