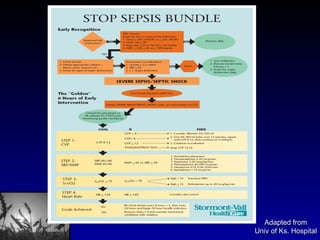
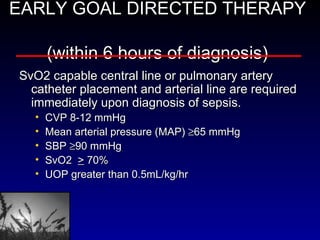
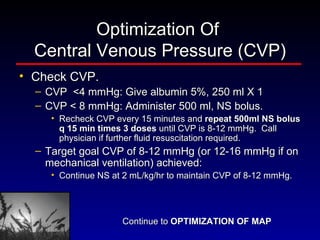
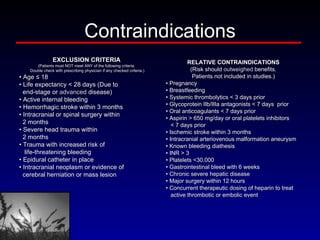
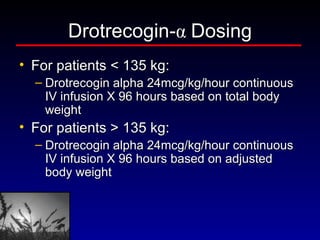
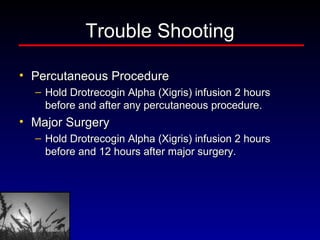
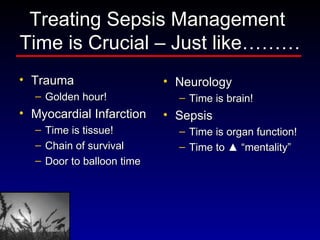
The document discusses sepsis treatment bundles which include early goal directed therapy, corticosteroids, antibiotics, ARDSnet ventilator management, stress ulcer prophylaxis, deep vein thrombosis prophylaxis, and Drotrecogin alpha. It provides details on the components, goals, and guidelines for each bundle element aimed at improving outcomes for patients with sepsis.