Downloaded 449 times



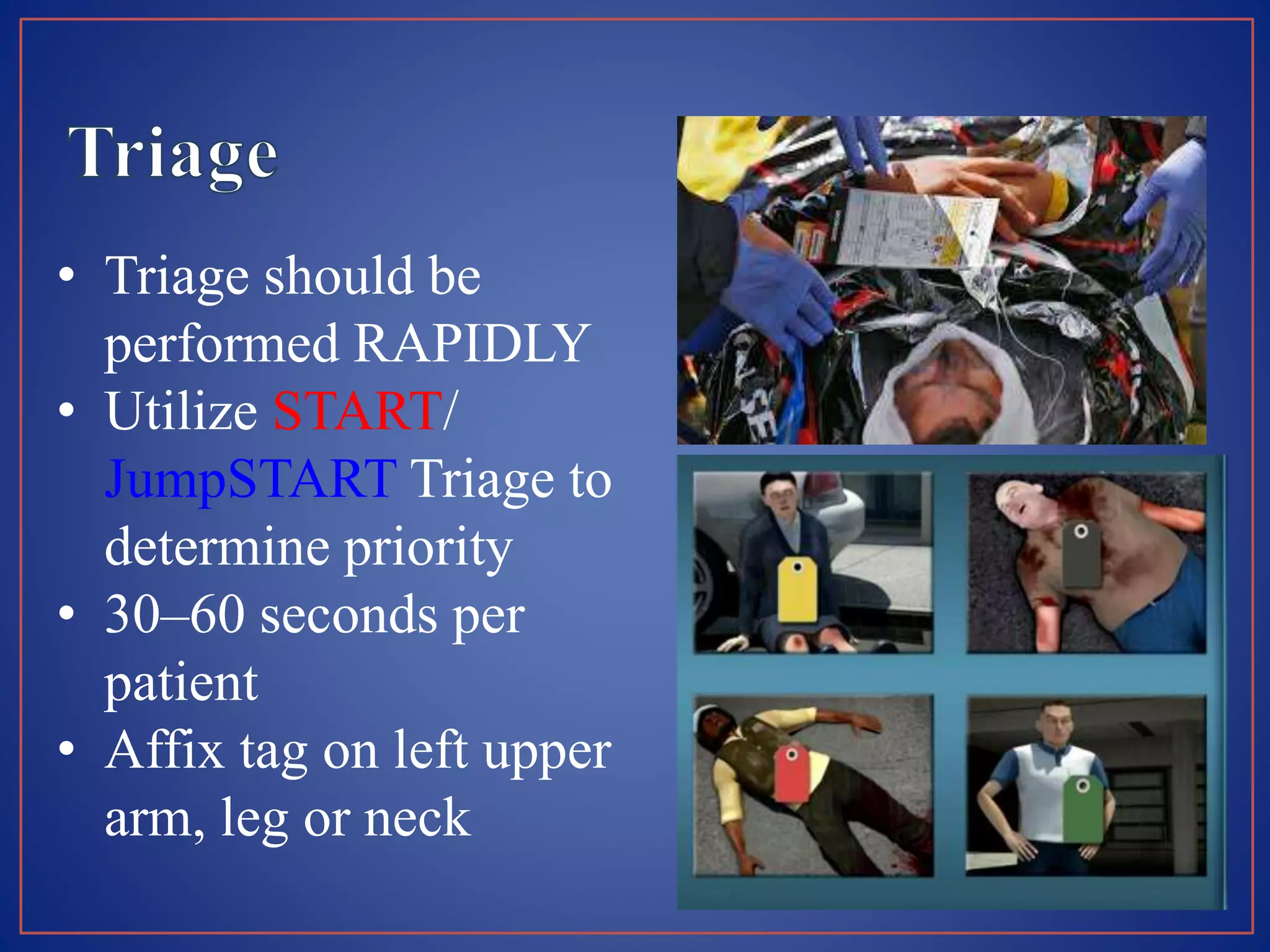


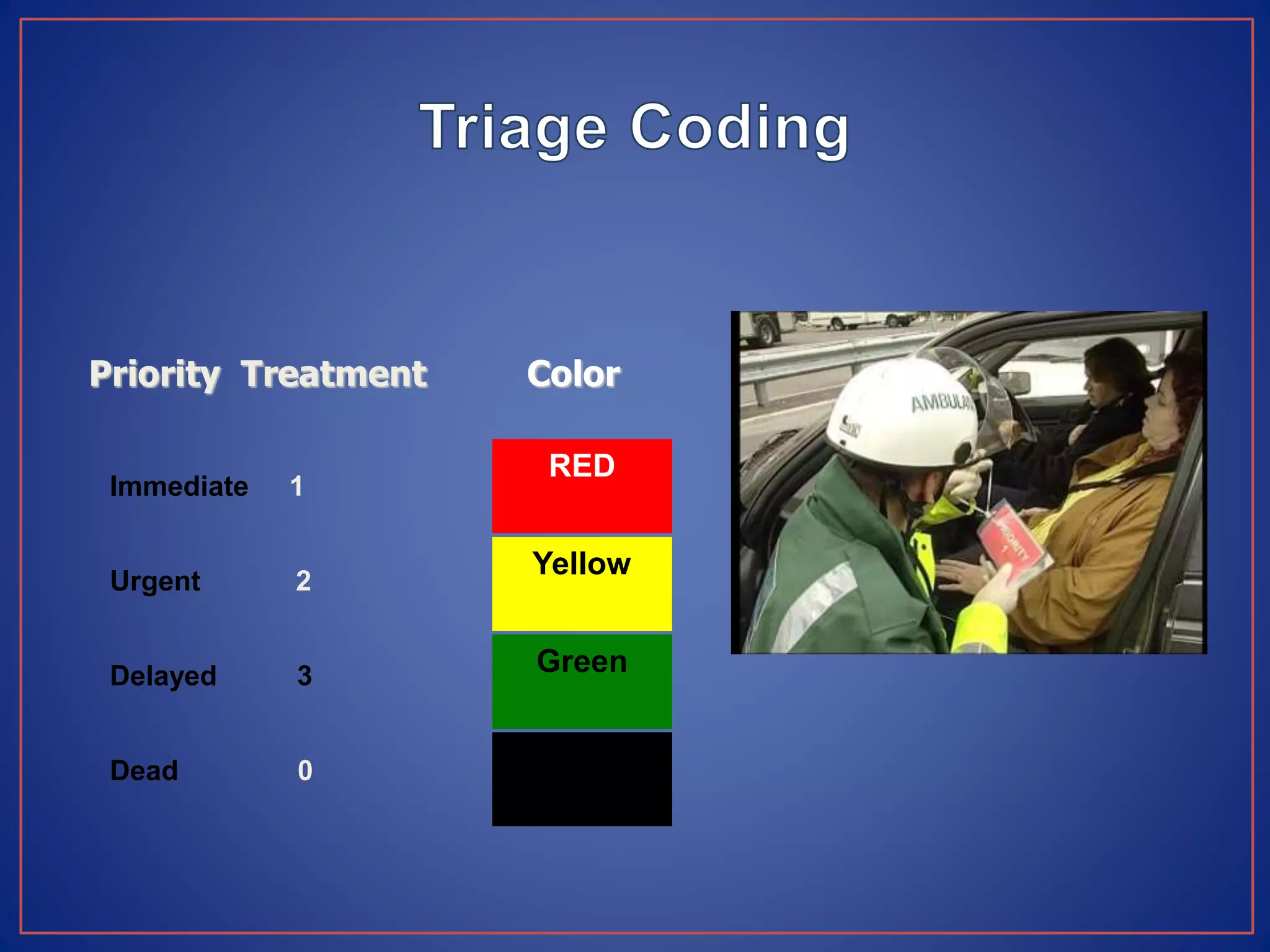


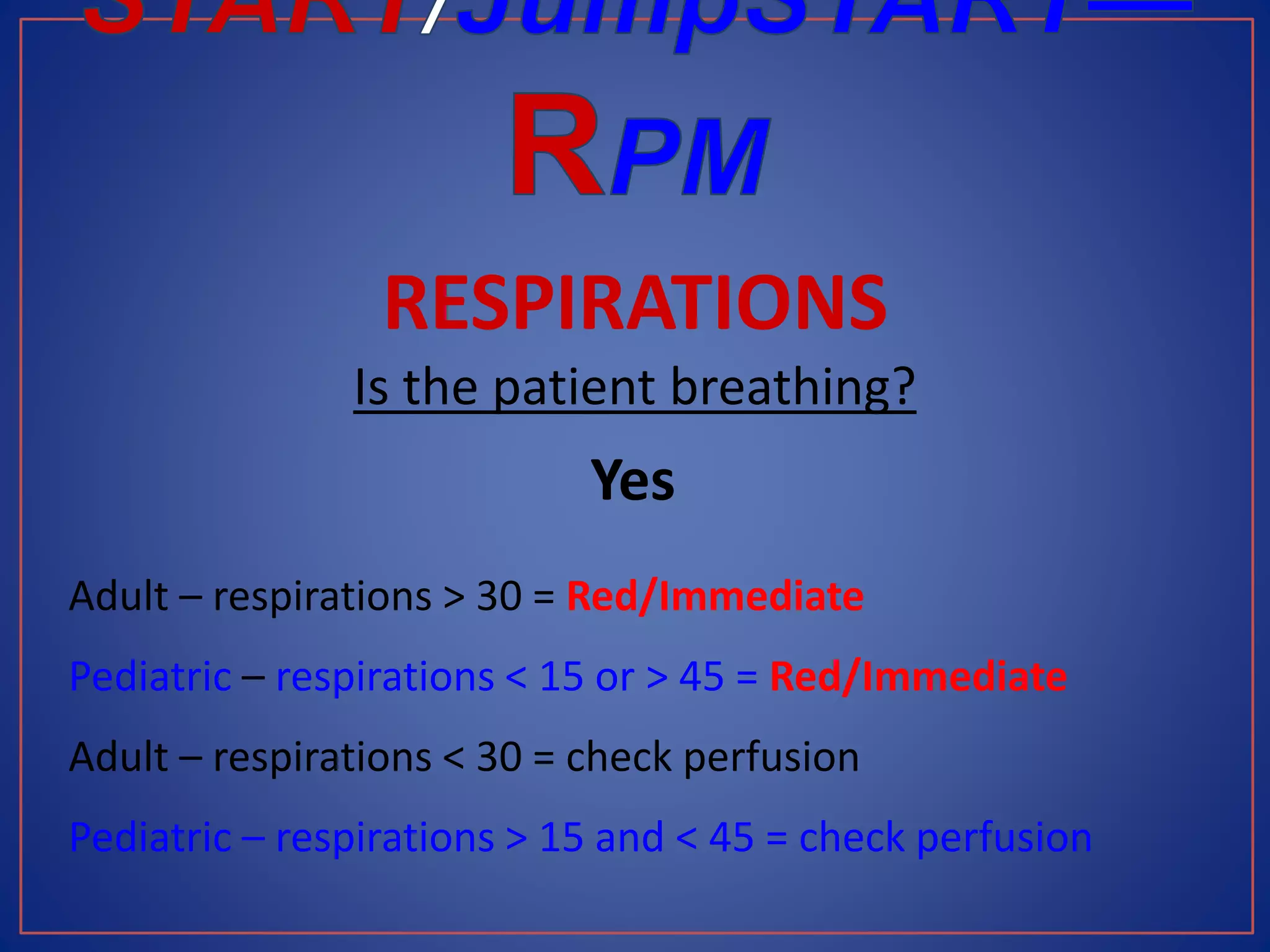
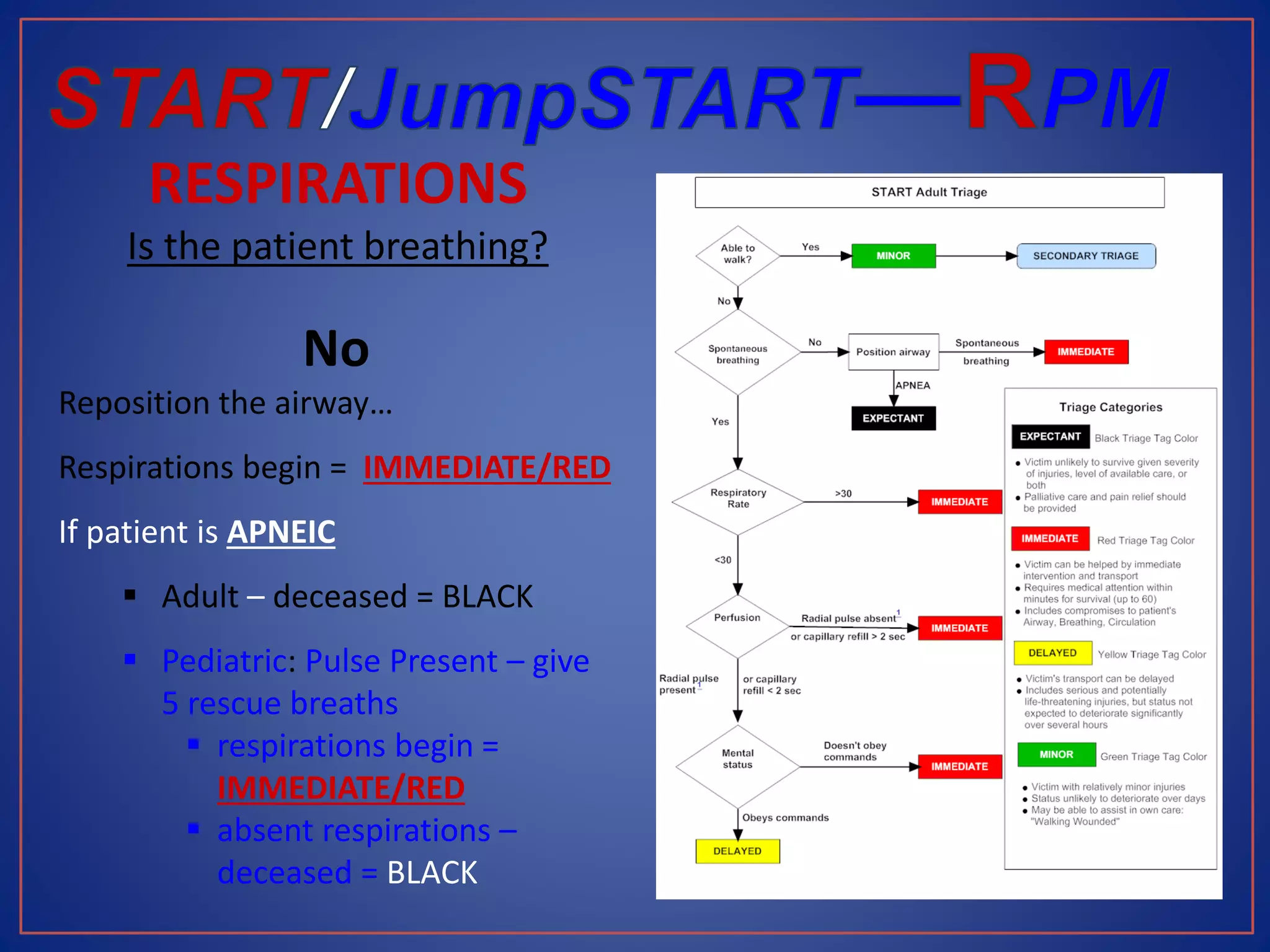
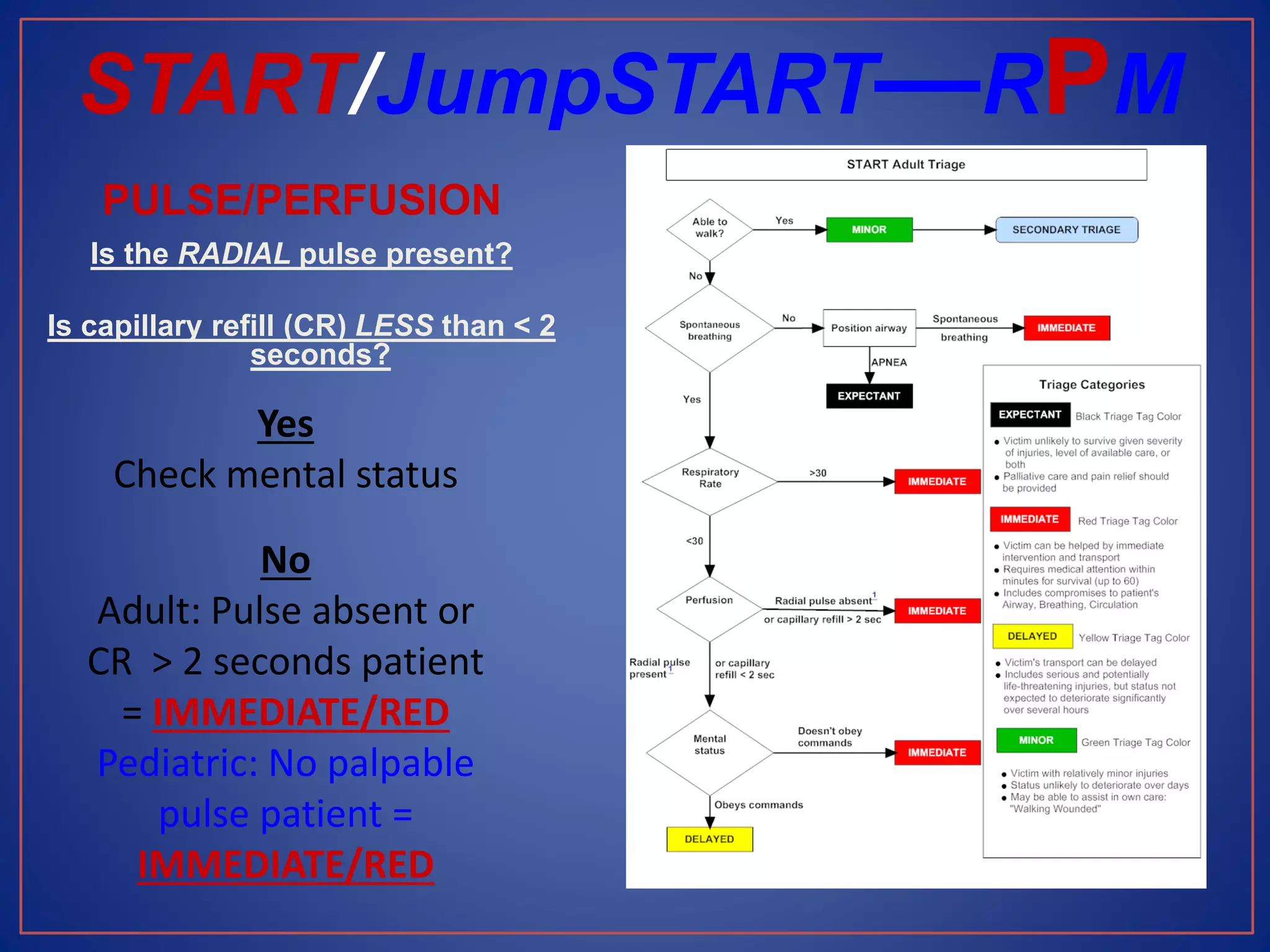
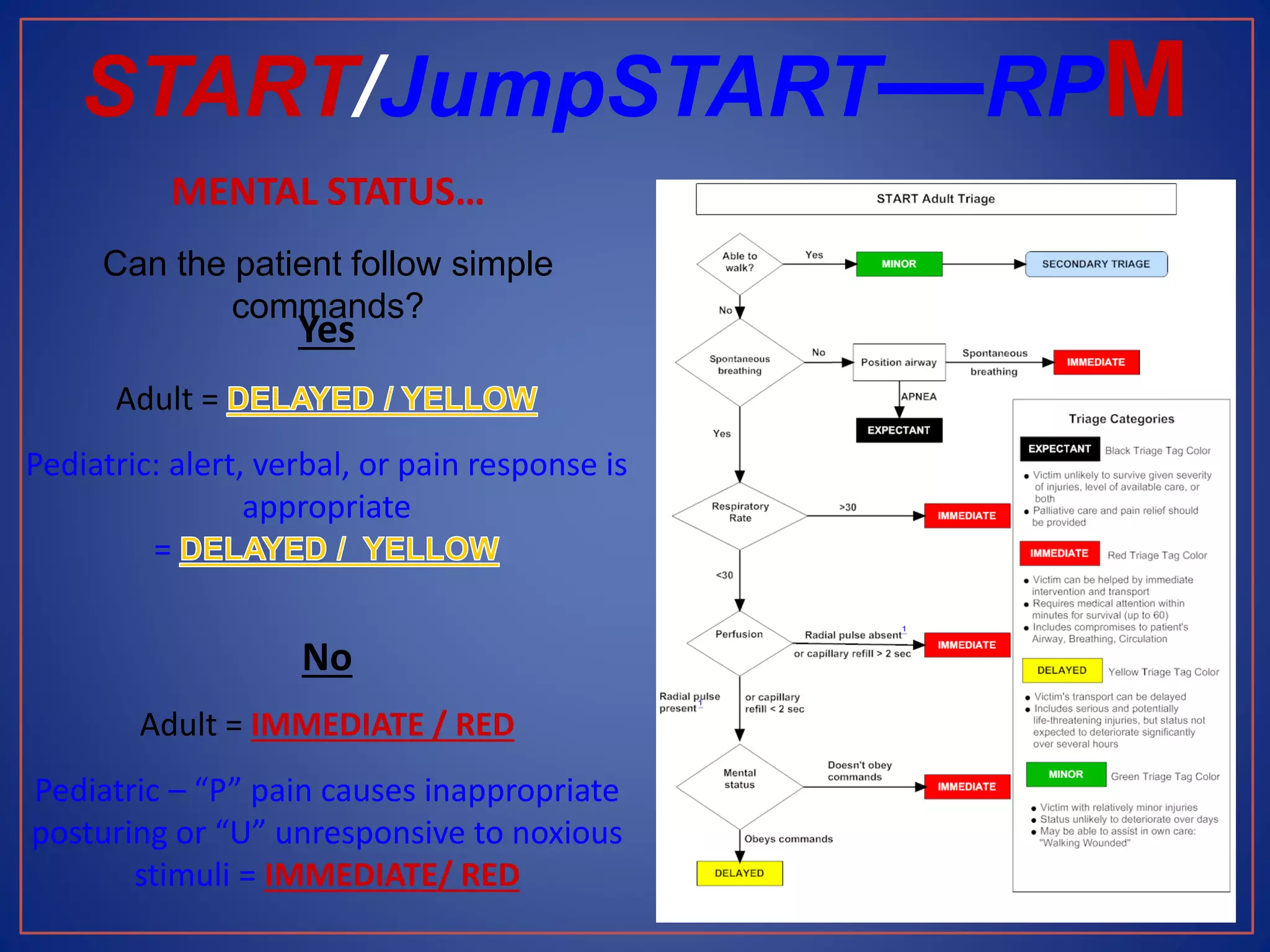
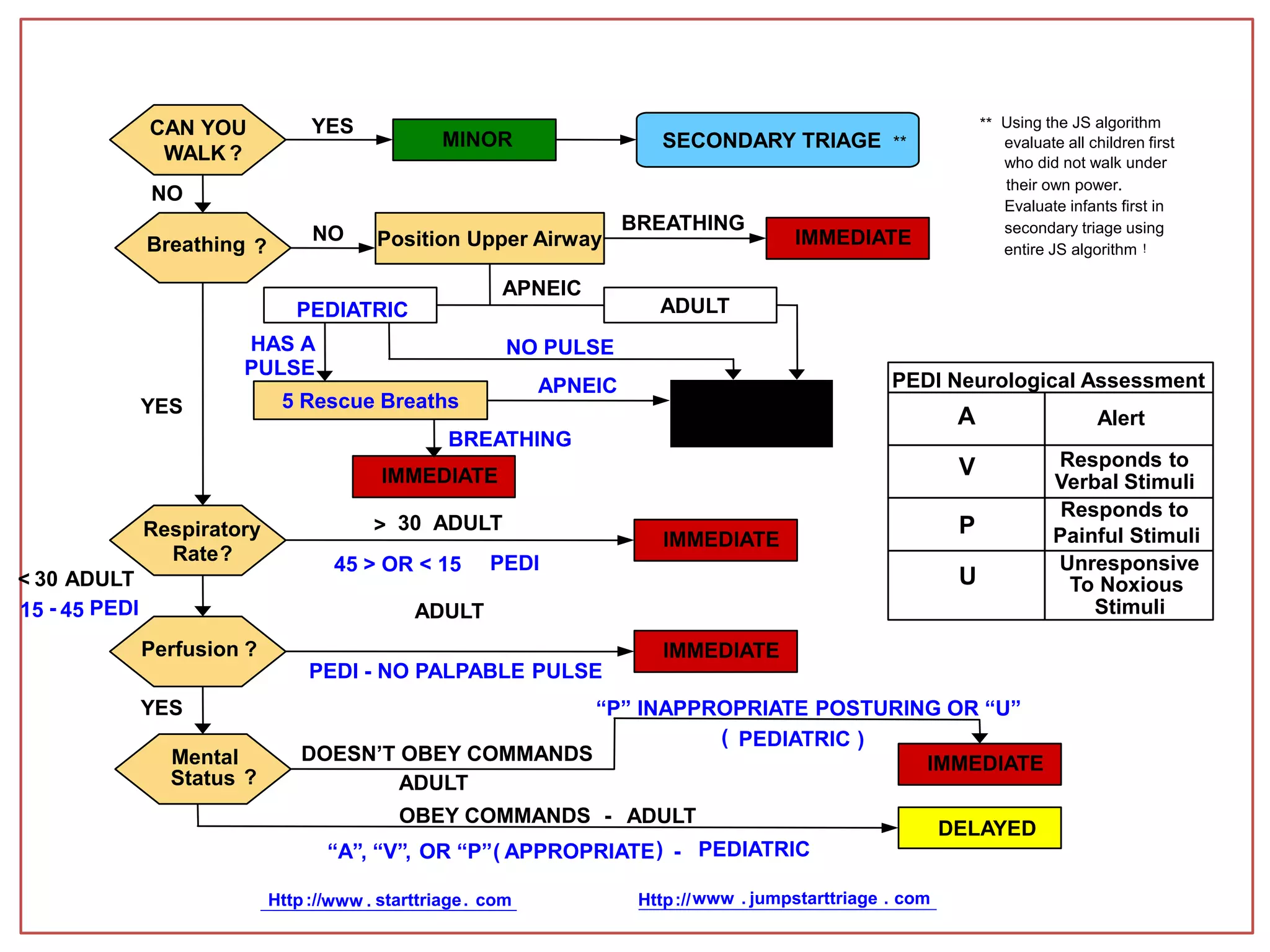
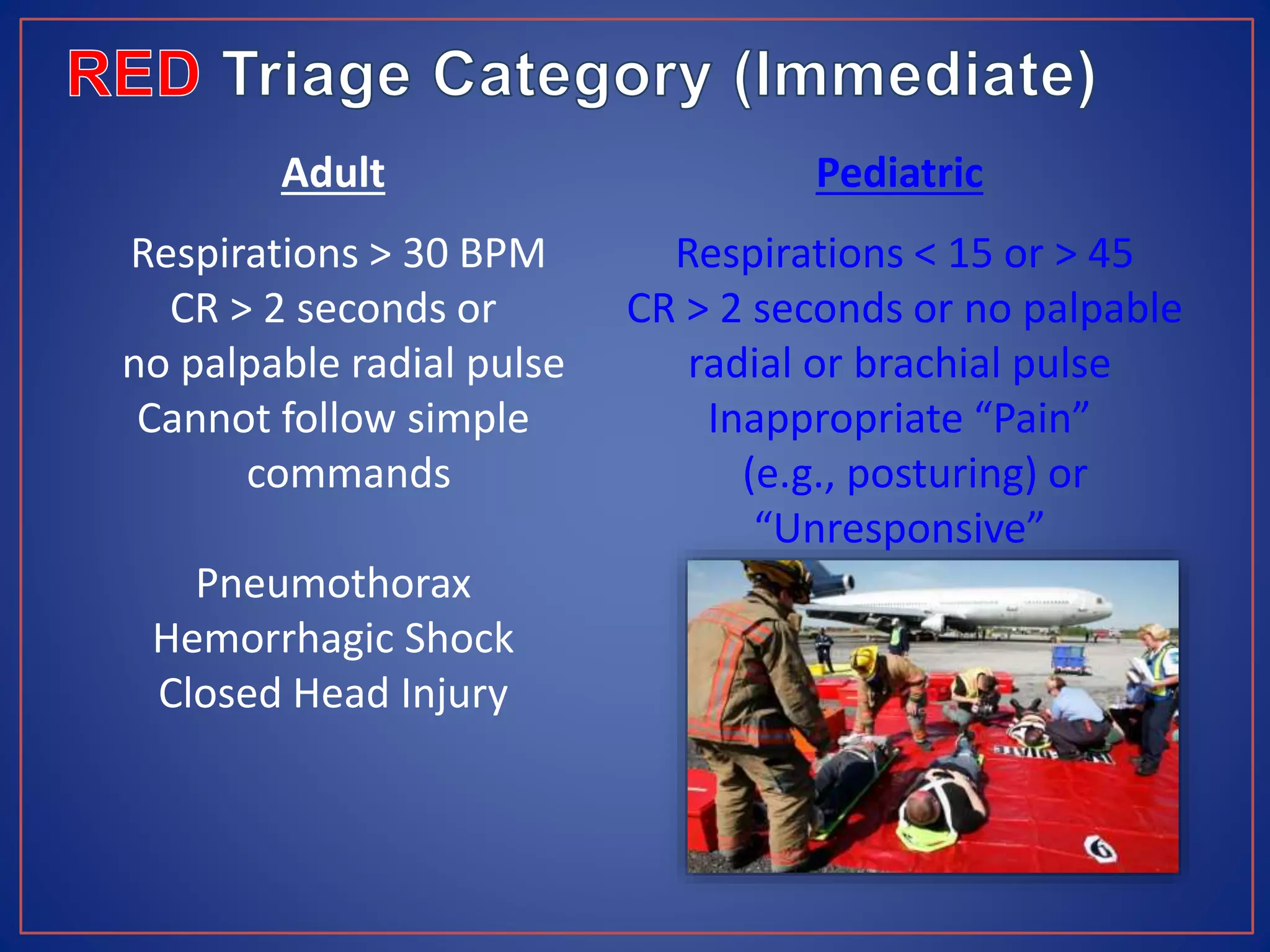





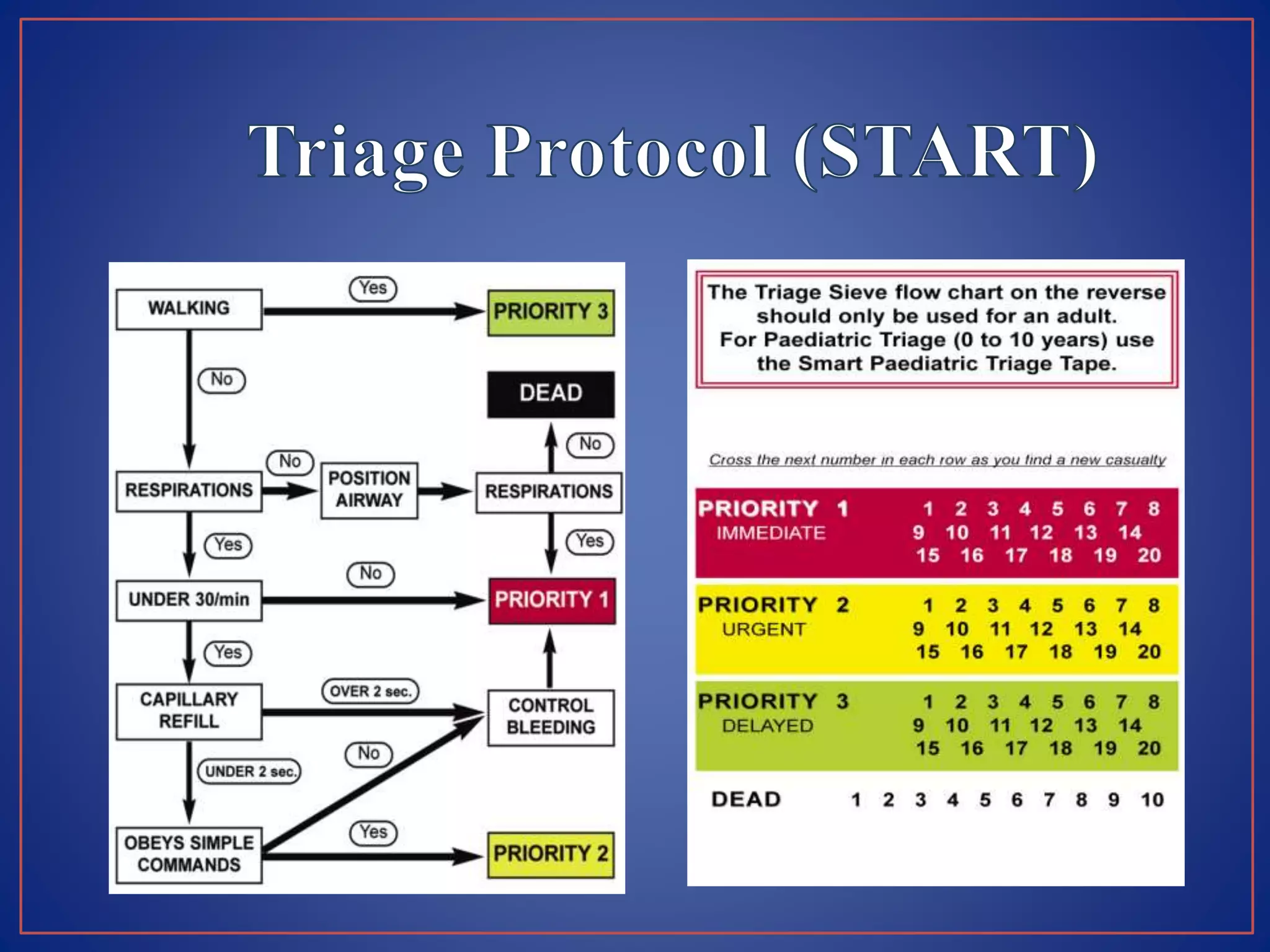
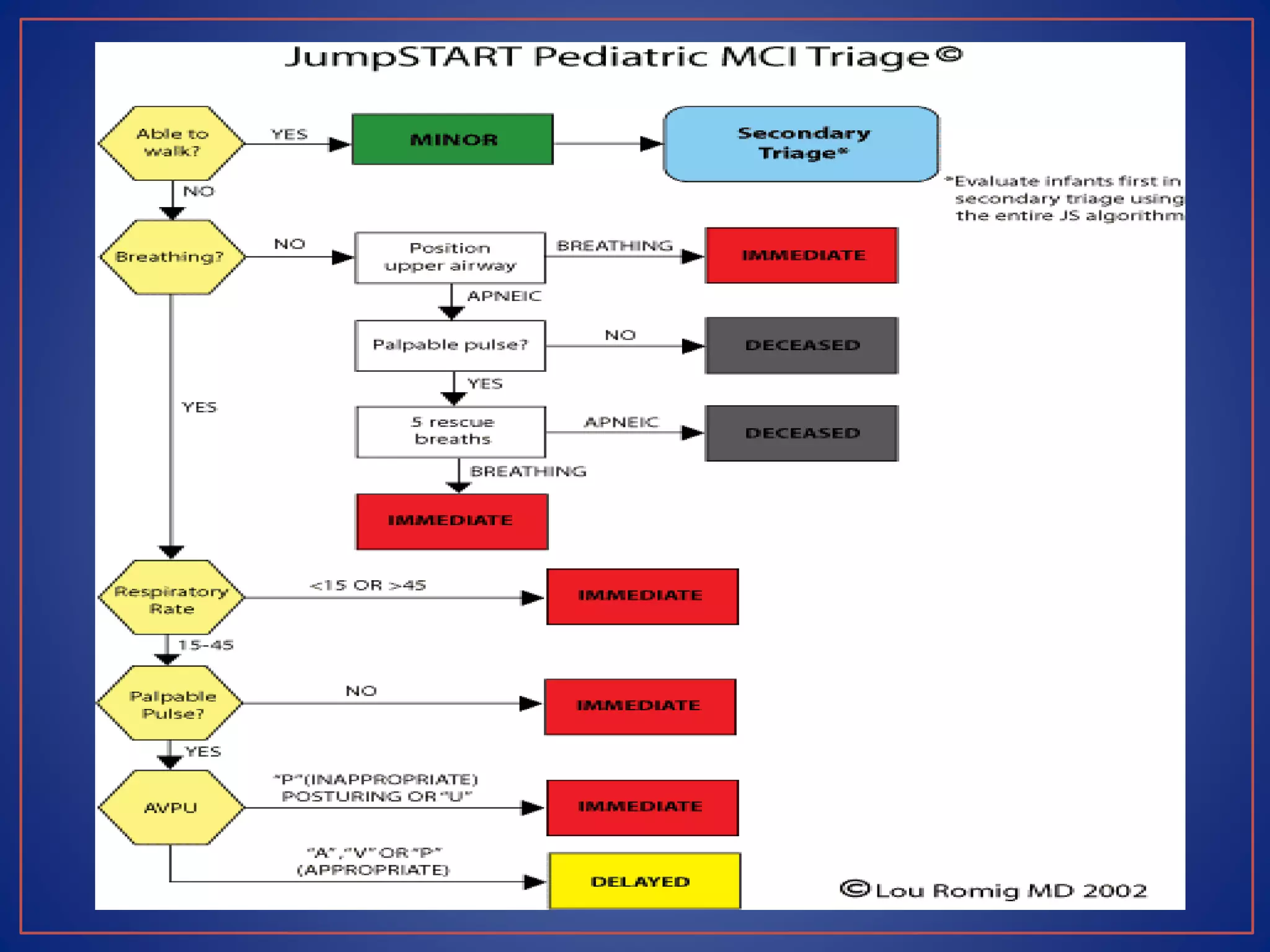













































This document provides information on triage systems and procedures. It defines triage as sorting patients based on treatment priority. The START and JumpSTART triage systems categorize patients as red/immediate, yellow/delayed, green/minor, or black/deceased based on their respiration, pulse, and mental status. It outlines how to rapidly assess and tag patients in a mass casualty event using these criteria in 3 sentences or less per patient to maximize survivability. The document recommends clearing walking patients first and prioritizing life-saving interventions for immediate patients before movement or additional treatment.























































































