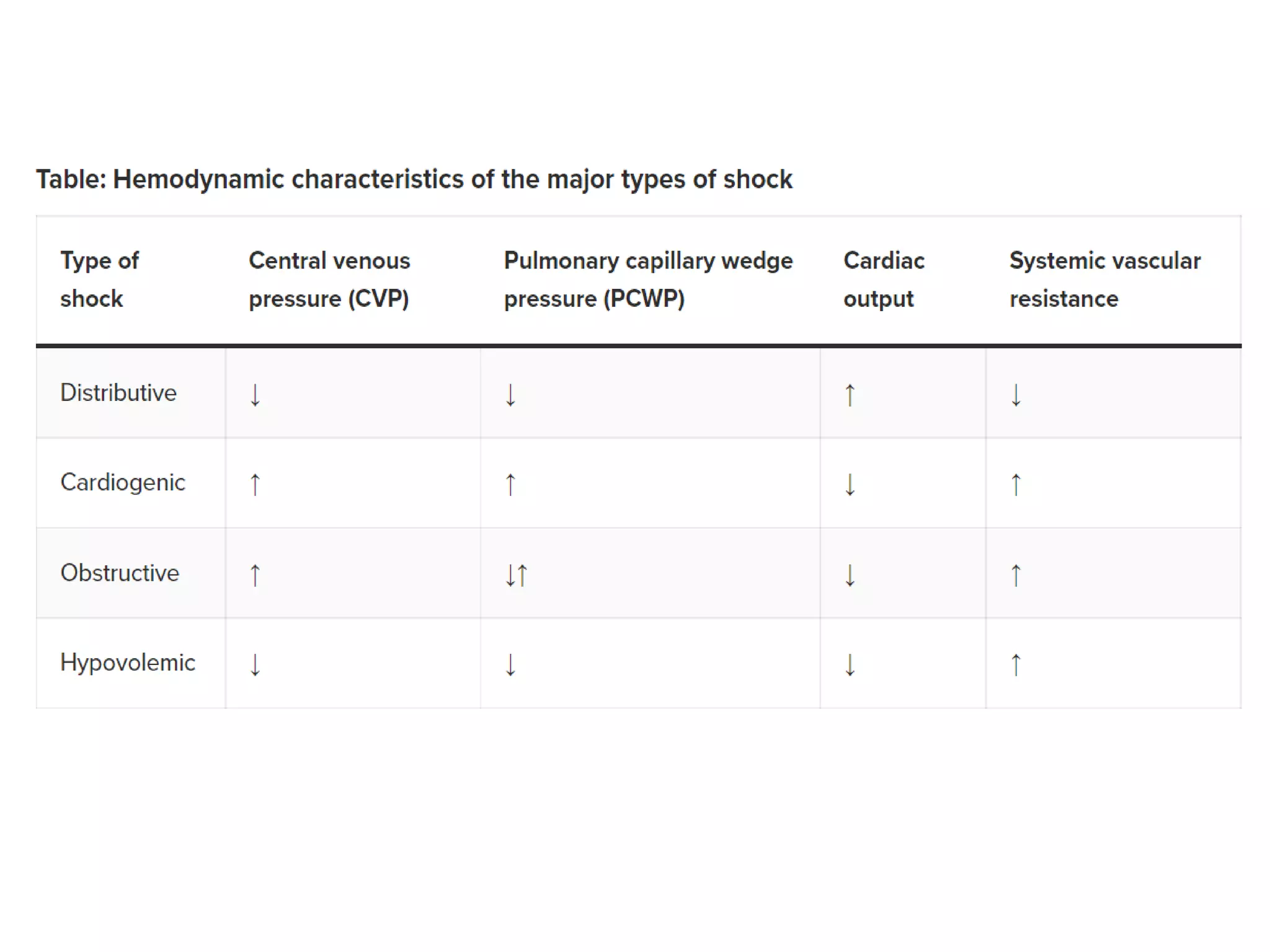
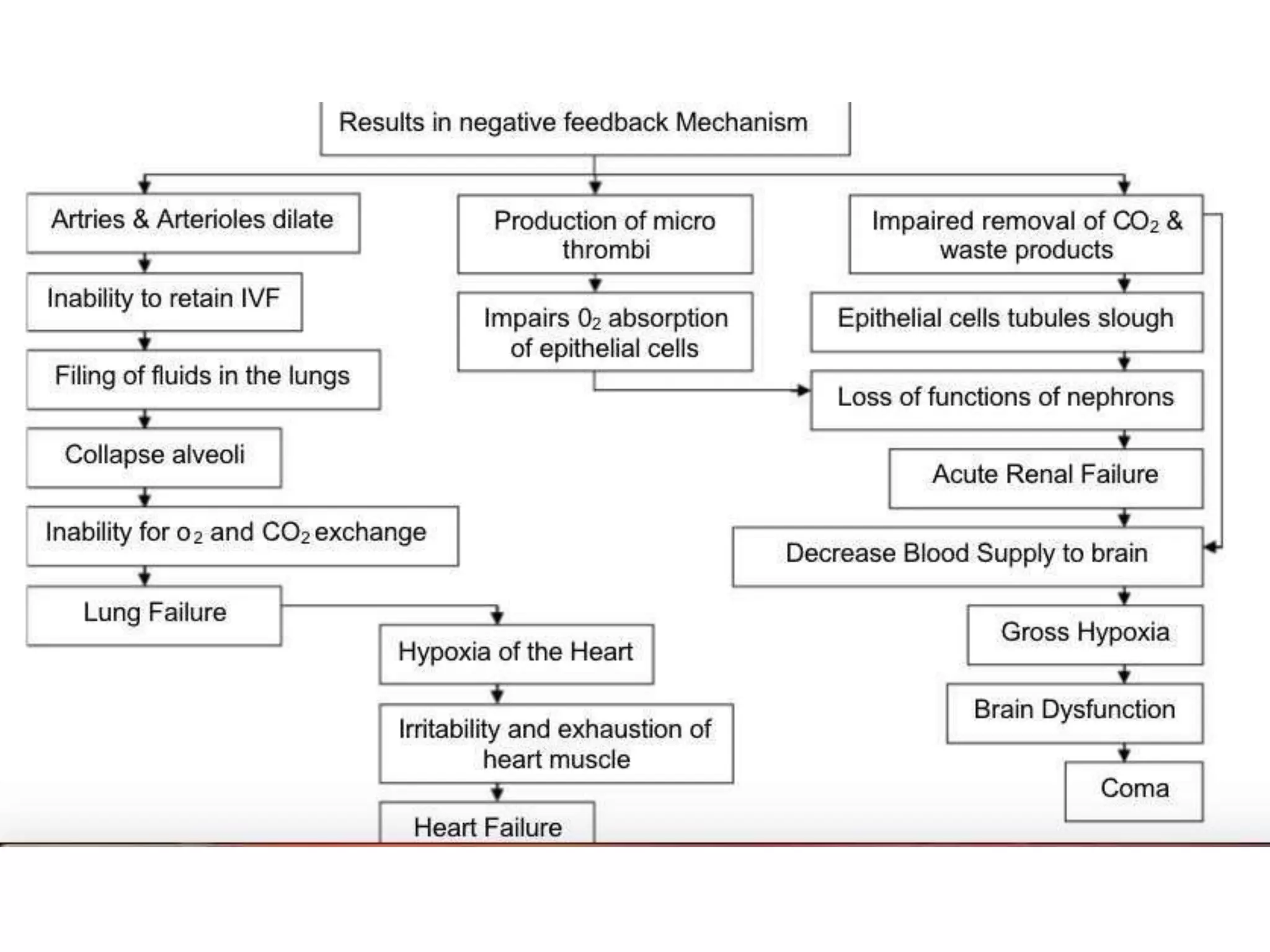
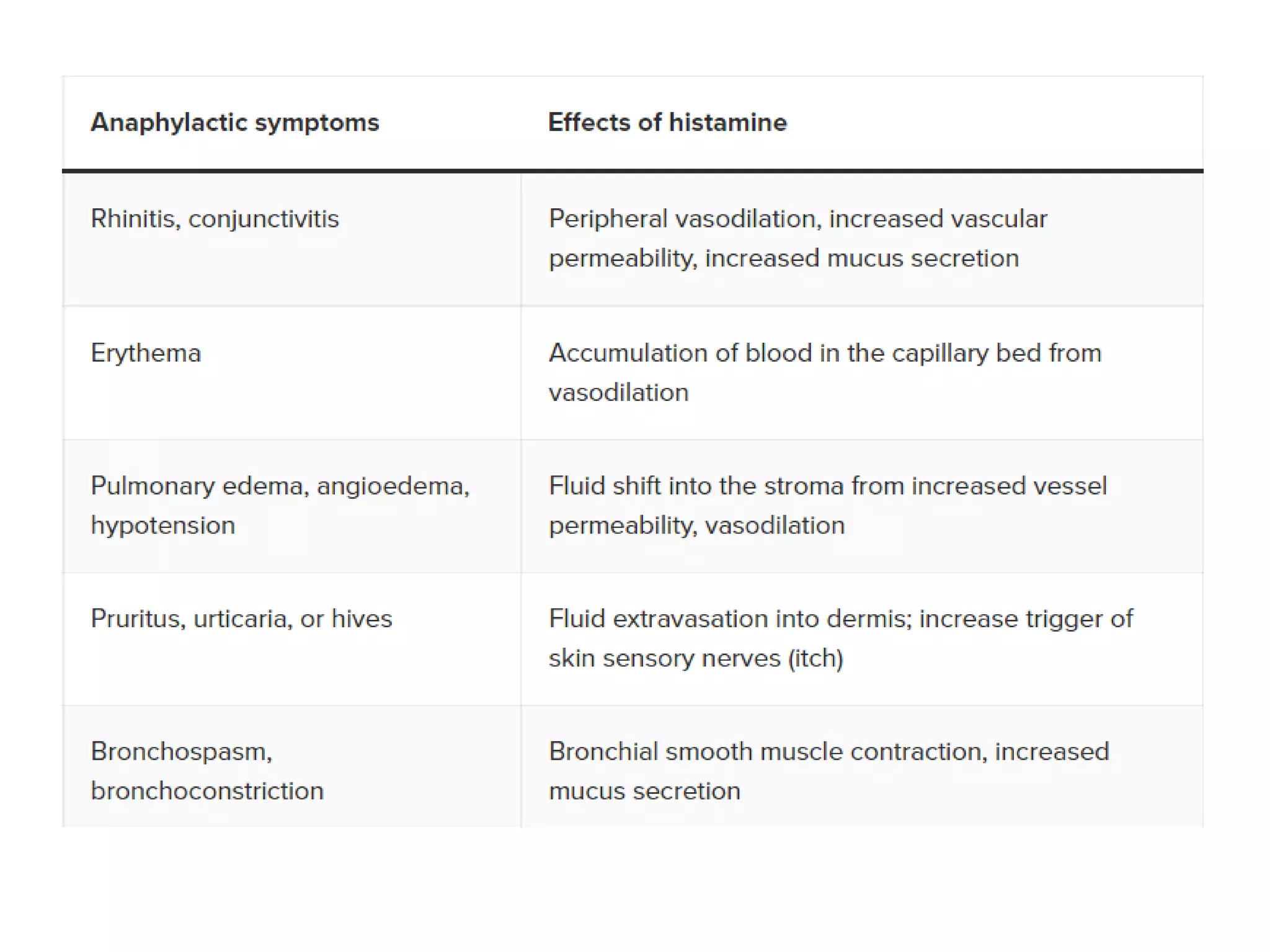
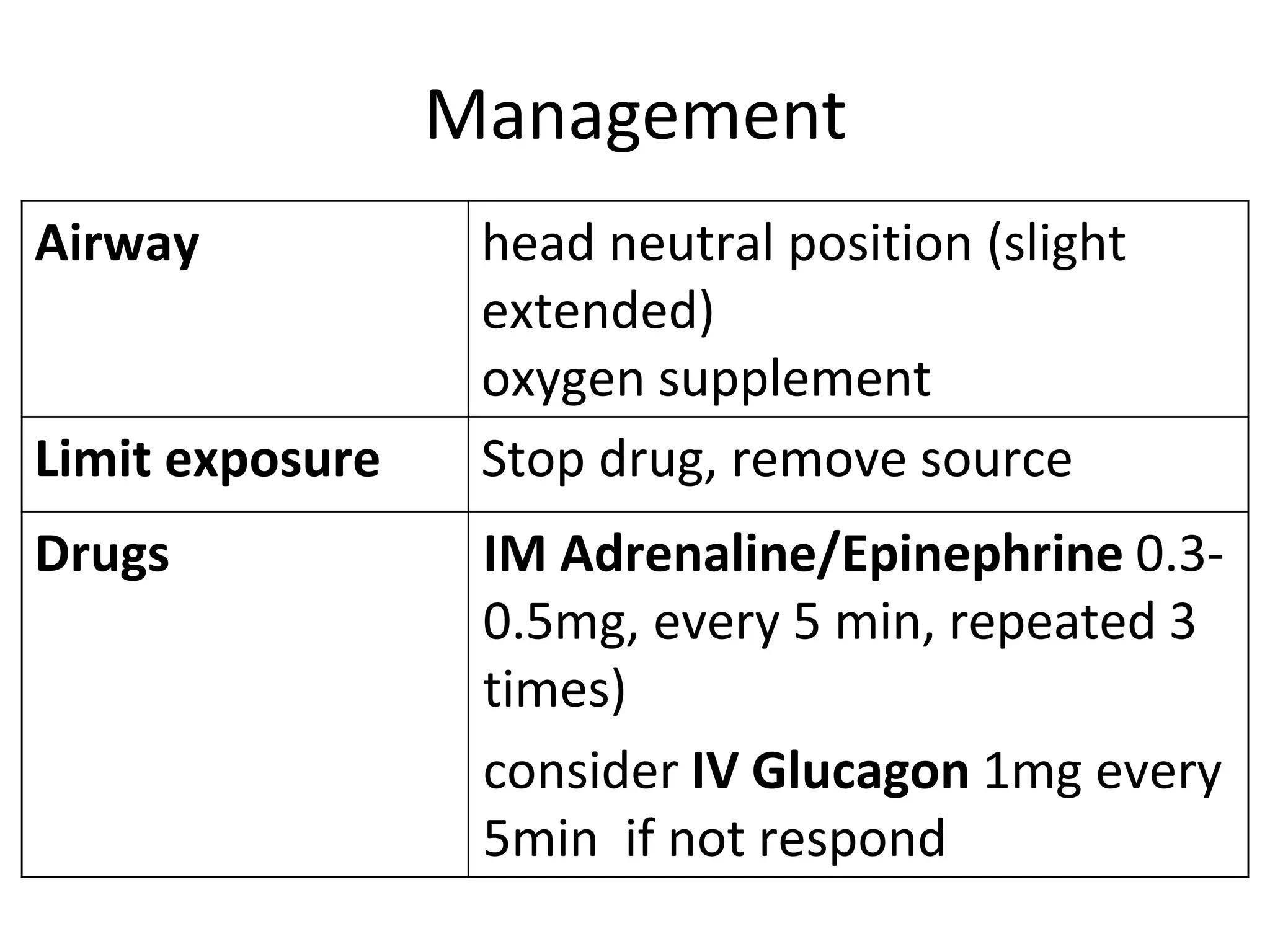
The document discusses distributive shock, focusing on its various forms including septic, anaphylactic, and neurogenic shock, highlighting their causes, symptoms, and management. It outlines the pathophysiology, diagnostic approaches, and treatment strategies for each type, emphasizing the importance of prompt intervention to prevent organ dysfunction and improve patient outcomes. Specific protocols for assessment, resuscitation, and pharmacological treatment using fluids and medications are provided, along with preventative measures.