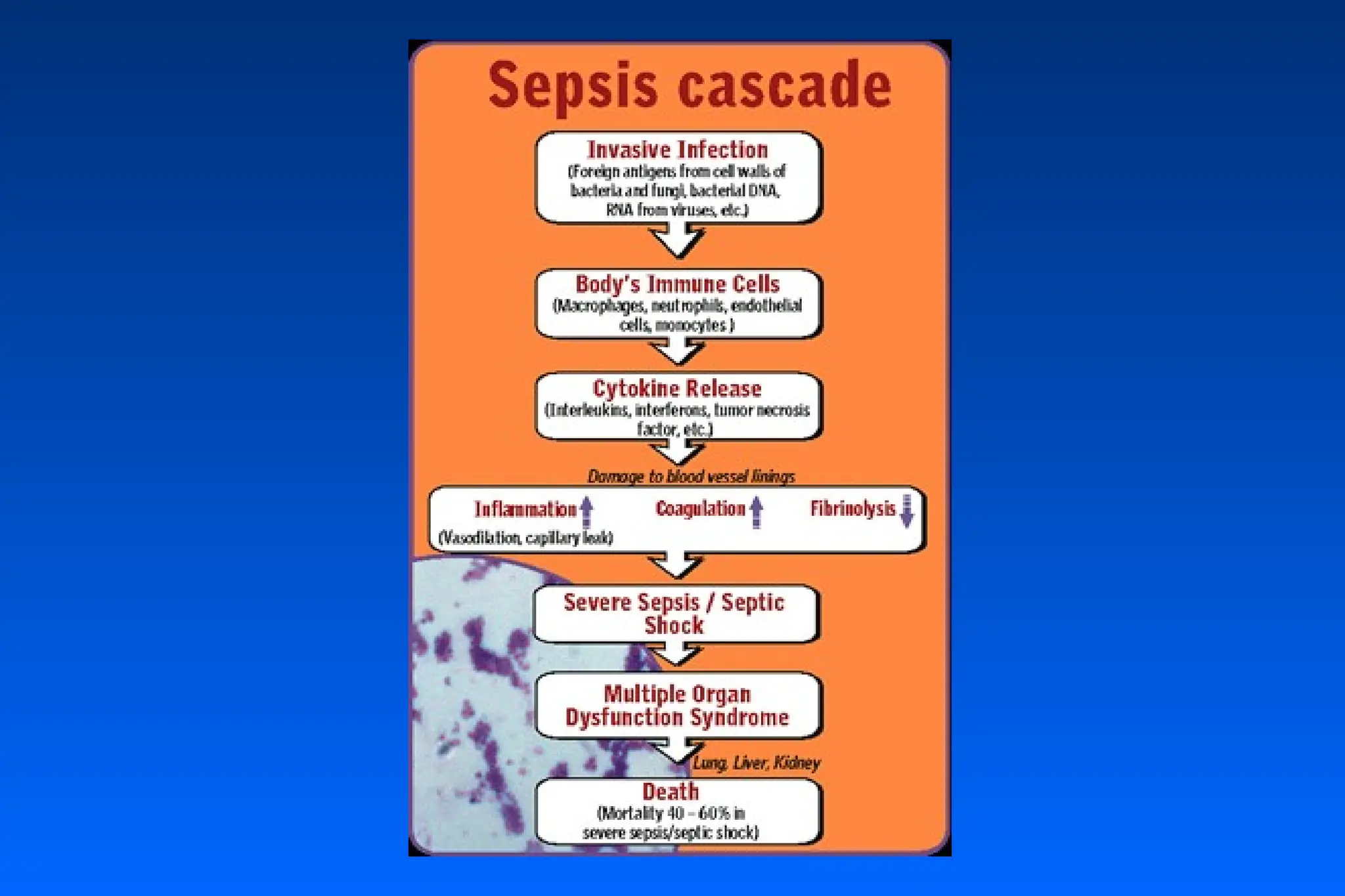
Sepsis Syndrome
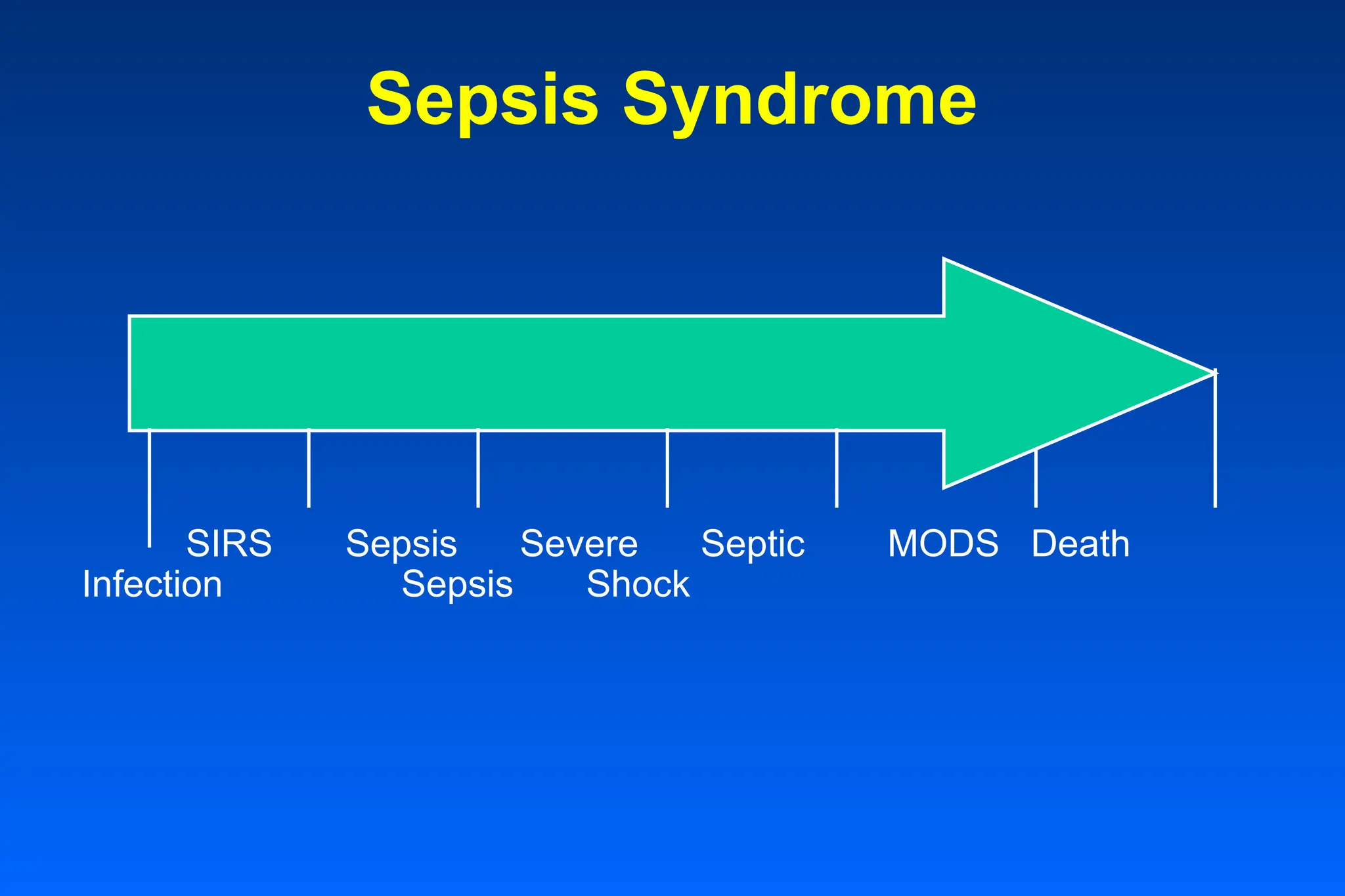
• Sepsisencompasses a spectrum of clinical conditions
caused by the immune response to infection and is
characterized by systemic inflammation and
coagulation.
• Sepsis includes the full range of responses from
systemic inflammatory response (SIRS) to organ
dysfunction to multiple organ failure and ultimately
death.
3.
Sepsis Morbidity &Mortality
• Leading cause of death in noncoronary ICU patients
• 13th leading cause of death in U.S.
• Over 500,000 episodes each year
• 35-70% mortality
• 20-50% positive blood cultures
• 40% hospital deaths after injury due to MODS
4.
Sepsis On TheRise
• Incidences projected to rise to 1.0 million cases
annually in the US within the next decade due to:
• Aging population
• Increased awareness and diagnosis
• Immunocompromised patients
• Invasive procedures
• Resistant pathogens
5.
SIRS Sepsis SevereSeptic MODS Death
Infection Sepsis Shock
Sepsis Syndrome
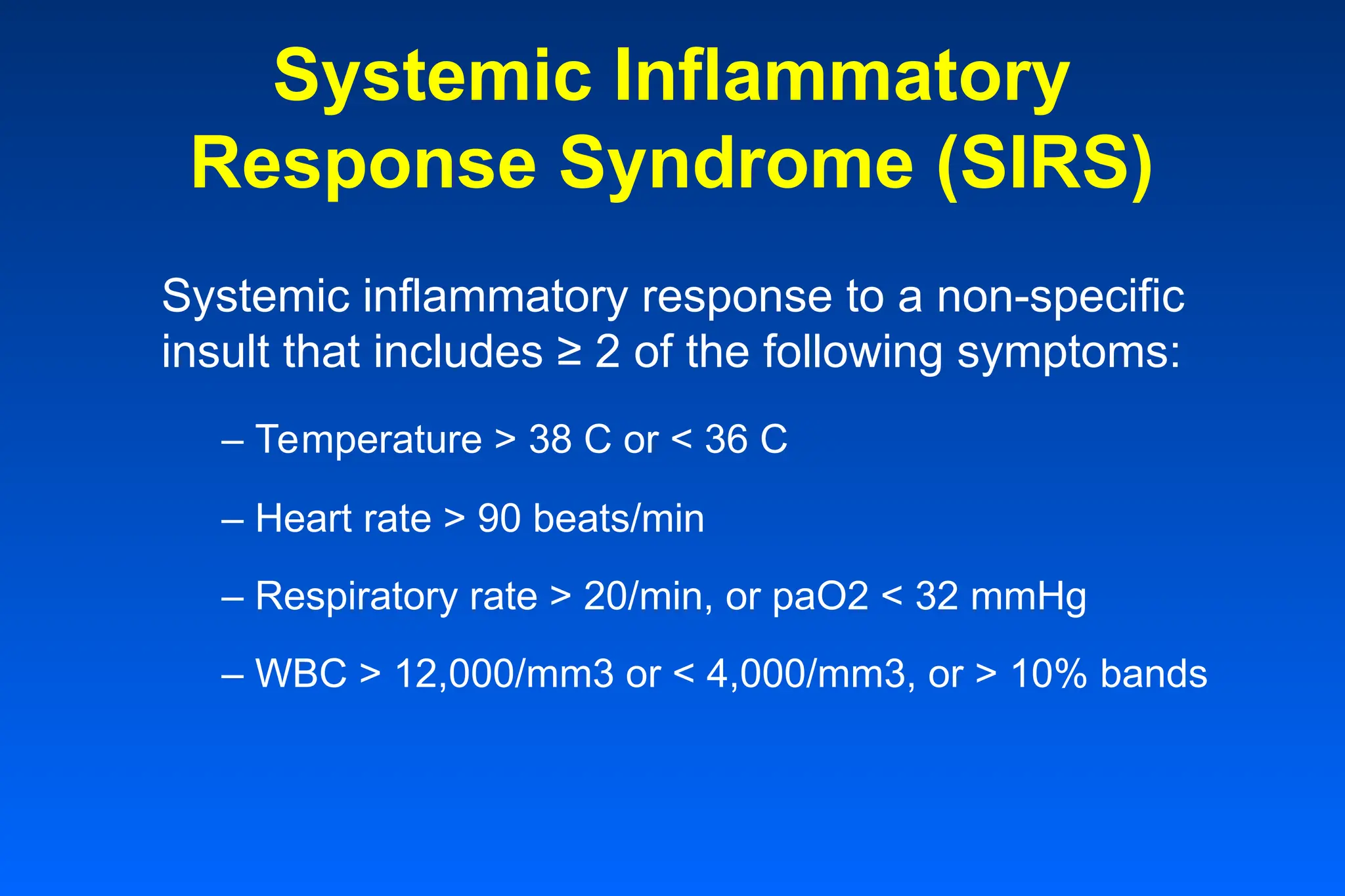
Systemic Inflammatory
Response Syndrome(SIRS)
Systemic inflammatory response to a non-specific
insult that includes ≥ 2 of the following symptoms:
– Temperature > 38 C or < 36 C
– Heart rate > 90 beats/min
– Respiratory rate > 20/min, or paO2 < 32 mmHg
– WBC > 12,000/mm3 or < 4,000/mm3, or > 10% bands
8.
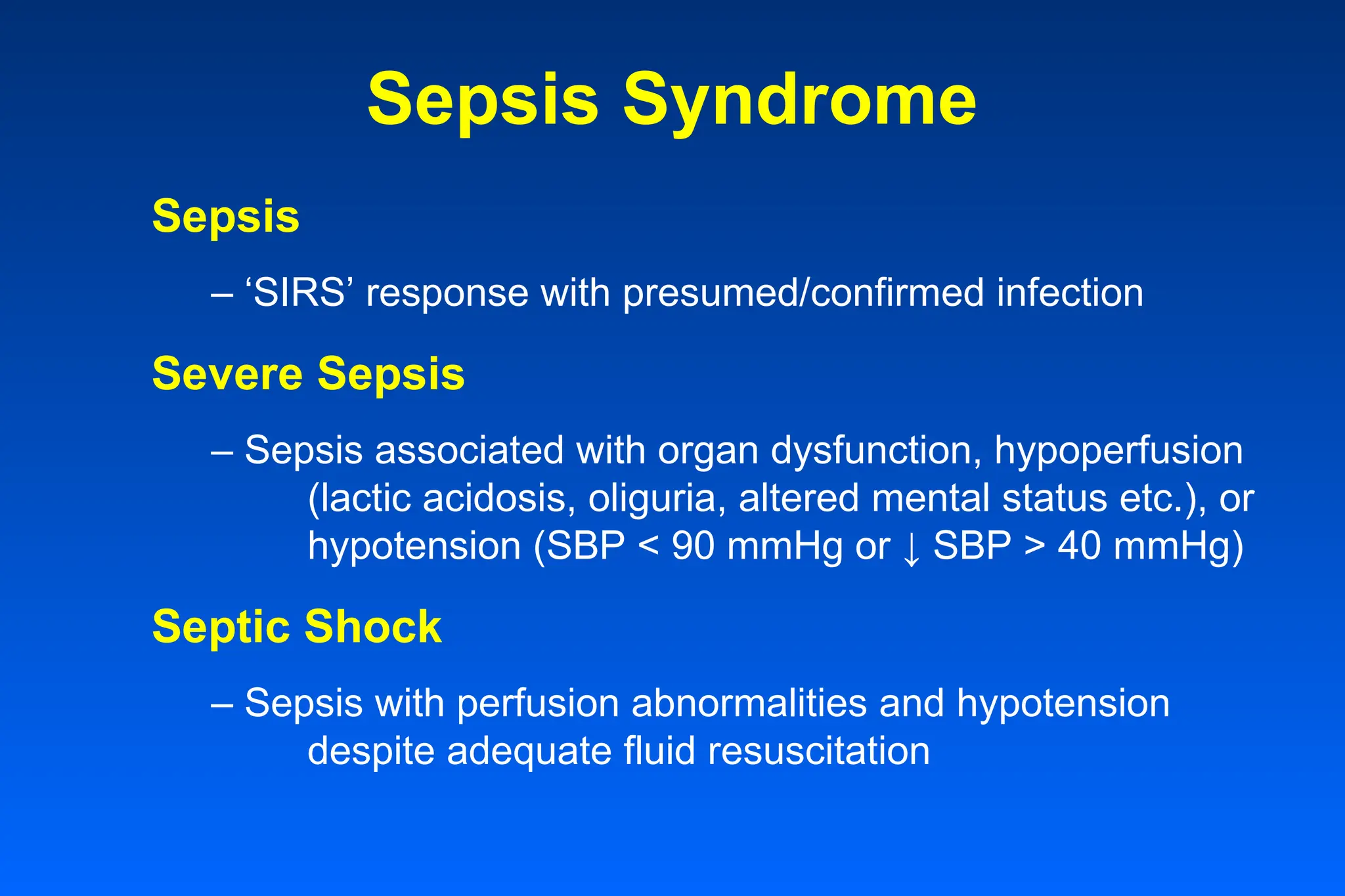
Sepsis Syndrome
Sepsis
– ‘SIRS’response with presumed/confirmed infection
Severe Sepsis
– Sepsis associated with organ dysfunction, hypoperfusion
(lactic acidosis, oliguria, altered mental status etc.), or
hypotension (SBP < 90 mmHg or ↓ SBP > 40 mmHg)
Septic Shock
– Sepsis with perfusion abnormalities and hypotension
despite adequate fluid resuscitation
9.
Multiple Organ Dysfunction
Syndrome(MODS)
Multiple Organ Failure
– Presence of severe dysfunction of at least
two organ system lasting for more than 24
hours.
– Four or more systems - mortality near to
100 percent
11.
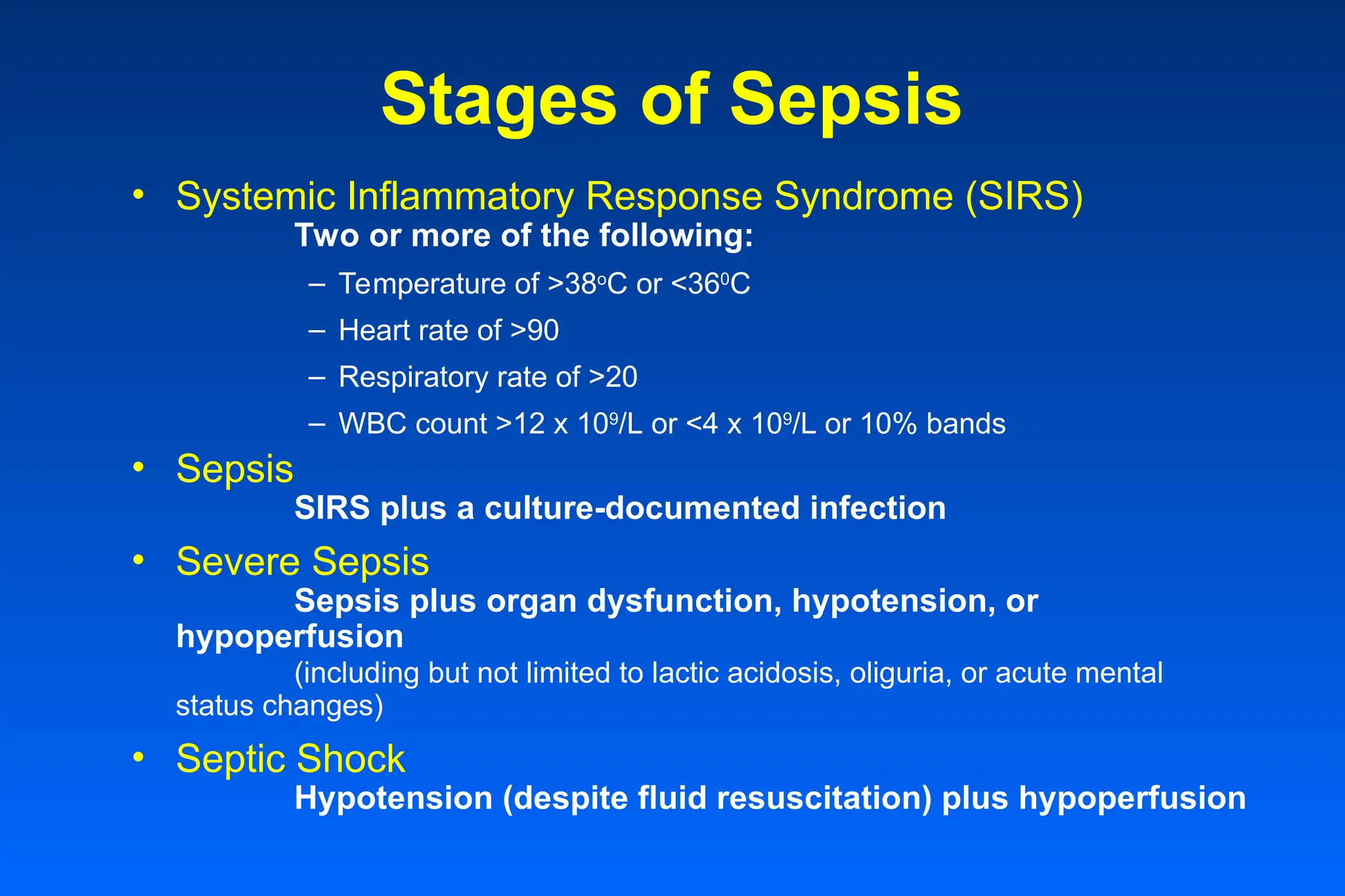
Stages of Sepsis
•Systemic Inflammatory Response Syndrome (SIRS)
Two or more of the following:
– Temperature of >38o
C or <360
C
– Heart rate of >90
– Respiratory rate of >20
– WBC count >12 x 109
/L or <4 x 109
/L or 10% bands
• Sepsis
SIRS plus a culture-documented infection
• Severe Sepsis
Sepsis plus organ dysfunction, hypotension, or
hypoperfusion
(including but not limited to lactic acidosis, oliguria, or acute mental
status changes)
• Septic Shock
Hypotension (despite fluid resuscitation) plus hypoperfusion
12.
Compensatory anti-inflammatory
response syndrome(CARS)
Overcompensating Anti-inflammatory Response
A syndrome in which anti-inflammatory mediator release
overcompensates for the systemic inflammatory response
leading to a state of immune suppression, increased
susceptibility to infection, and impaired recovery.
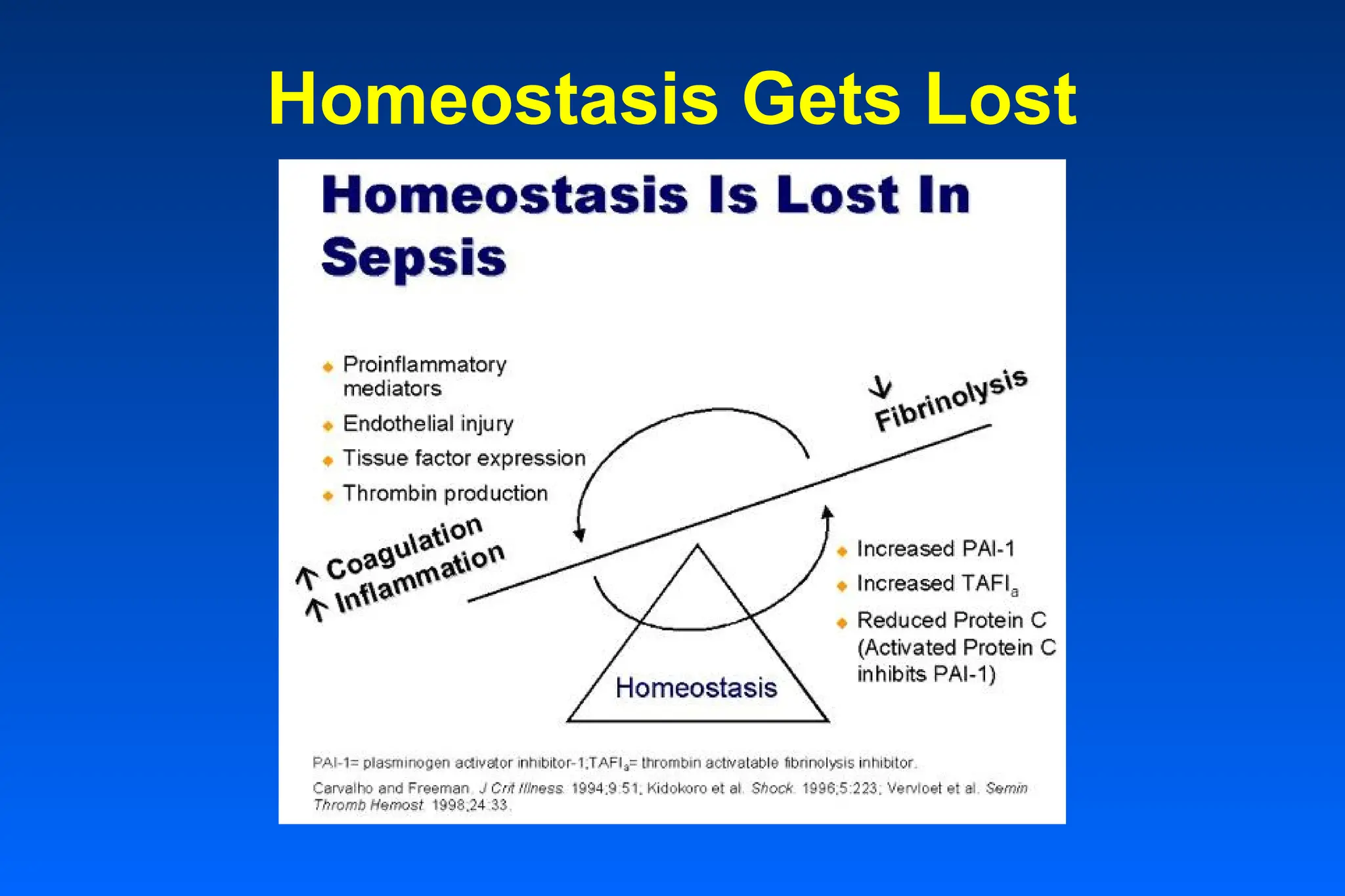
Systemic Response
• Initialsystemic response
• Release of cytokines from the inflammatory system
• Inflammation
• Initiation of coagulation abnormalities
• Activation of coagulation
• Inhibition of fibrinolysis
• Platelet activation
• Activation of secondary systems
• Complement system, contact system, multiple cytokines and
chemical mediators, free oxygen radicals, and nitric oxide.
18.
Inflammatory Cascade
• Pro-inflammatorycytokines promote endothelial cell
adhesion, induce the release of free radicals and activate the
coagulation cascade
• Anti-inflammatory mediators provide a negative feedback
mechanism for inflammatory and coagulation reactions.
• If an imbalance develops between SIRS and CARS,
homeostasis is violated:
• If SIRS predominates the result may be sepsis/
severe sepsis/ septic shock.
• If CARS predominates, the immune system may be
suppressed, leaving the patient susceptible to life-
threatening infections.
20.
Coagulation Cascade
• Coagulationcascade
• Activation of coagulation
• Inhibition of fibrinolysis
• Potentates the inflammation cascade
21.
Impaired Fibrinolysis
• ImpairedFibrinolysis
• Fibrinolysis is the breakdown of clots
• Normally activated with coagulation
• Fibrinolysis suppressed in sepsis
23.
Sepsis Mediators
• Myocardialdepressant factor(s)
• Enkephalins
• Adrenocorticoid hormone
• Prekallikrein
• Interleukin-1
• Cytokinines (acid metabolites) (eg,
leukotrienes, prostaglandins,
thromboxanes)
• The coagulation cascade
• The complement system
• The fibrinolytic system
• Histamines
• Bradykinins
• Catecholamines
• Glucocorticoids
• Tumor necrosis factor
• Beta-endorphins
The following systems and mediators are stimulated in sepsis:
Treatment for Sepsis
3.Improve Perfusion
– Prevent organ dysfunction
2. Treat The Cause
– Seek primary site of infection
– Direct therapy to primary cause
1. Stabilize The Patient
– Fluids (lots of fluids)
– Vasoconstrictors
42.
Treatment for
Warm Phase– Cold Phase
• Warm (Hyper-dynamic) Phase
– Fluids (lots of fluids)
– Find & Treat cause
– Vasoconstrictors
• Cold (Hypo-dynamic) Phase
– Fluids (treat hypovolemic shock)
– Continue treating cause
• Treat Early
– Mortality increases sharply the later the treatment
43.
Treatment Summary
1. Antibiotics(early administration)
2. Hemodynamic support
– Fluid Resuscitation
Restore tissue perfusion
Normalize cellular metabolism
– Vasopressor agents
Dopamine, Norepinephrine,
Dobutamine
3. Xigris (Activated Protein C)
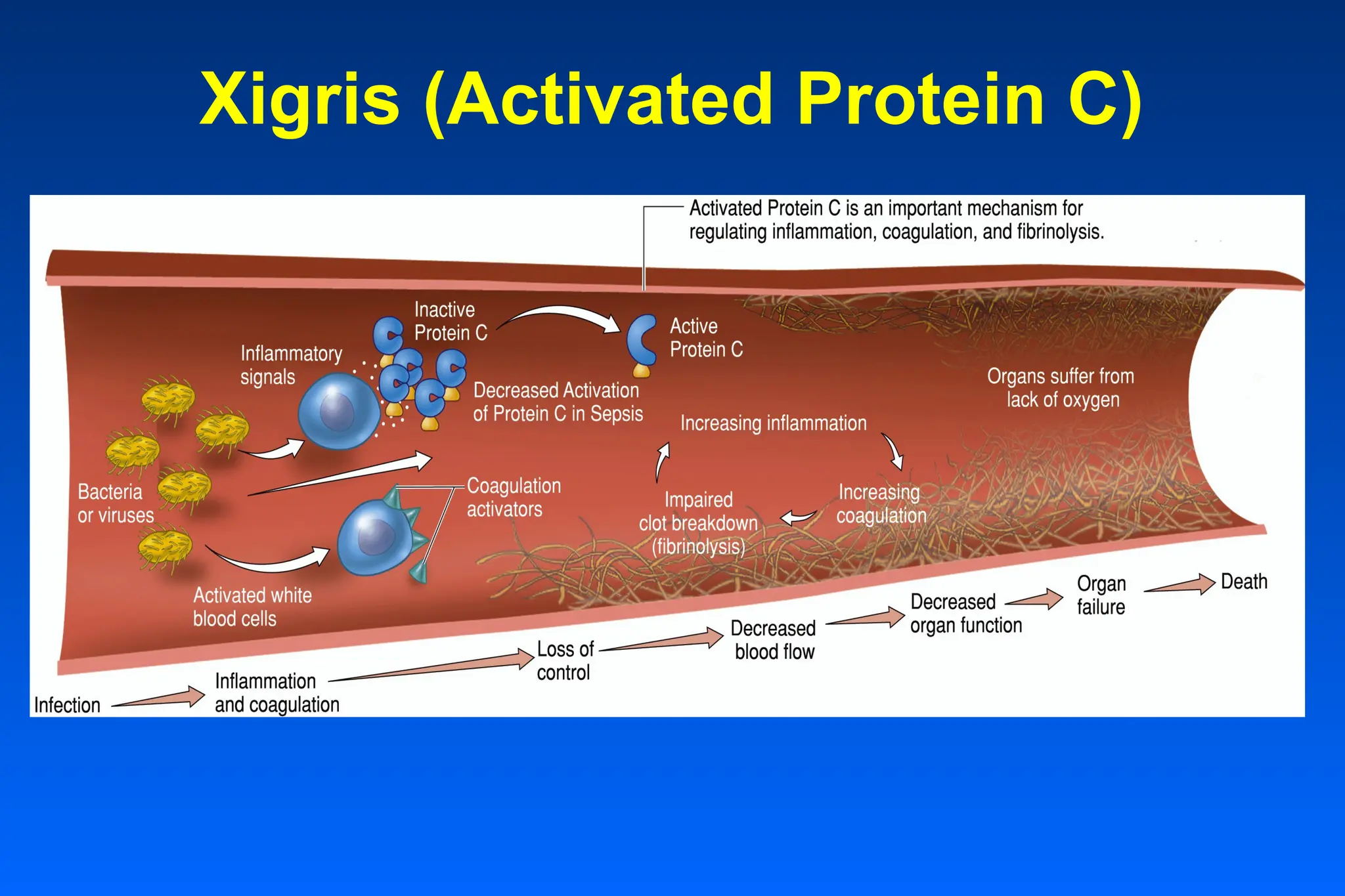
Activated Protein C(Xigris)
Mediates many actions of body homeostasis:
• suppression of inflammation
• prevention of microvascular coagulation
• reversal of impaired fibrinolysis
46.
Xigris Facts
1. Xigrishas a short half-life
2. Xigris should be discontinued 2 hours prior to
performing an invasive surgical procedure
3. Immediately stop the administration of Xigris if
clinically important bleeding occurs.
47.
Xigris Contraindications
Xigris iscontraindicated in patients with the following
clinical situations:
• Active internal bleeding
• Recent—within 3 months—hemorrhagic stroke
• Recent—within 2 months—intracranial or intraspinal
surgery, or severe head trauma
• Trauma with increased risk of life-threatening bleeding
• Presence of an epidural catheter
• Intracranial neoplasm or mass lesion or evidence of cerebral
herniation
• Known hypersensitivity to drotrecogin alfa (activated) or any
component of this product
Vasopressin & SepticShock
Proposed Mechanisms
• Vasopressin levels in septic shock may be inappropriately low and
contribute to hypotension
• Vasopressin blunts the vasodilatory response from NO by reducing
synthesis of iNO synthase, and blocks KATP channels in smooth muscle
• Vasopressor action of vasopressin is increased in autonomic failure (eg.
septic shock)
• Vasopressin potentiates vasoconstrictor effects of norepinephrine
1. American Collegeof Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis
and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med 1992;20:864-74.
2. Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: analysis of incidence,
outcome, and associated costs of care. Crit Care Med 2001;29:1303-10.
3. Bone RC, Grodzin CJ, Balk RA. Sepsis: a new hypothesis for pathogenesis of the disease process. Chest 1997;112:235-
43.
4. Rangel-Frausto MS, Pittet D, Costigan M, et al. The natural history of the systemic inflammatory response syndrome
(SIRS): a prospective study. JAMA 1995;272:117-23.
5. Vervloet MG, Thijs LG, Hack CE. Derangements of coagulation and fibrinolysis in critically ill patients with sepsis and
septic shock. Semin Thromb Hemost 1998;24:33-44.
6. Kuhl DA. Current strategies for managing the patient with sepsis. Am J Health-Syst Pharm 2002;59(suppl 1):S9-13.
7. Bernard GR, Vincent J, Laterre P, et al. Efficacy and safety of recombinant human activated protein C for severe sepsis.
N Engl J Med 2001;344:699-709.
8. Drotrecogin alfa (activated) (Xigris), Eli Lilly and Company, 2004 (prescribing information).
9. Centers for Disease Control. Increase in national hospital discharge survey rates for septicemia—United States, 1979-
1987. JAMA 1990; 263: 937-8.
10. Balk RA. Severe sepsis and septic shock. Critical Care Clinics.2000; 2: 179-92.
11. American College of Chest Physicians/Society of Critical Care Medicine. Definitions for sepsis and organ failure and
guidelines for the use of innovative therapies in sepsis. Crit Care Med 1992; 20: 864-74.
12. Bernard et al. A recent definition of severe sepsis. N. Engl. J Med 2001; 344: 699-709.
13. Matuschak GM. Multiple systems organ failure: clinical expression, pathogenesis, and therapy, in Hall JB, Schmidt GA,
Wood LDH: Principles of Critical Care, McGraw-Hill, New York, 1992.
14. Wheeler AP, Bernard GR. Treating patients with severe sepsis. N Engl J Med 1999; 340: 207-13.
References
Editor's Notes
#2 We needed to come up with consistent definitions
to ensure accurate diagnoses
to ensure accurate record keeping (statistics)
to deliver the most appropriate and best care possible
The joint consensus conference between the American College of Chest Physicians (ACCP) and the Society of Critical Care Medicine (SCCM) standardized the terminology of sepsis and its sequelae in 1991 .
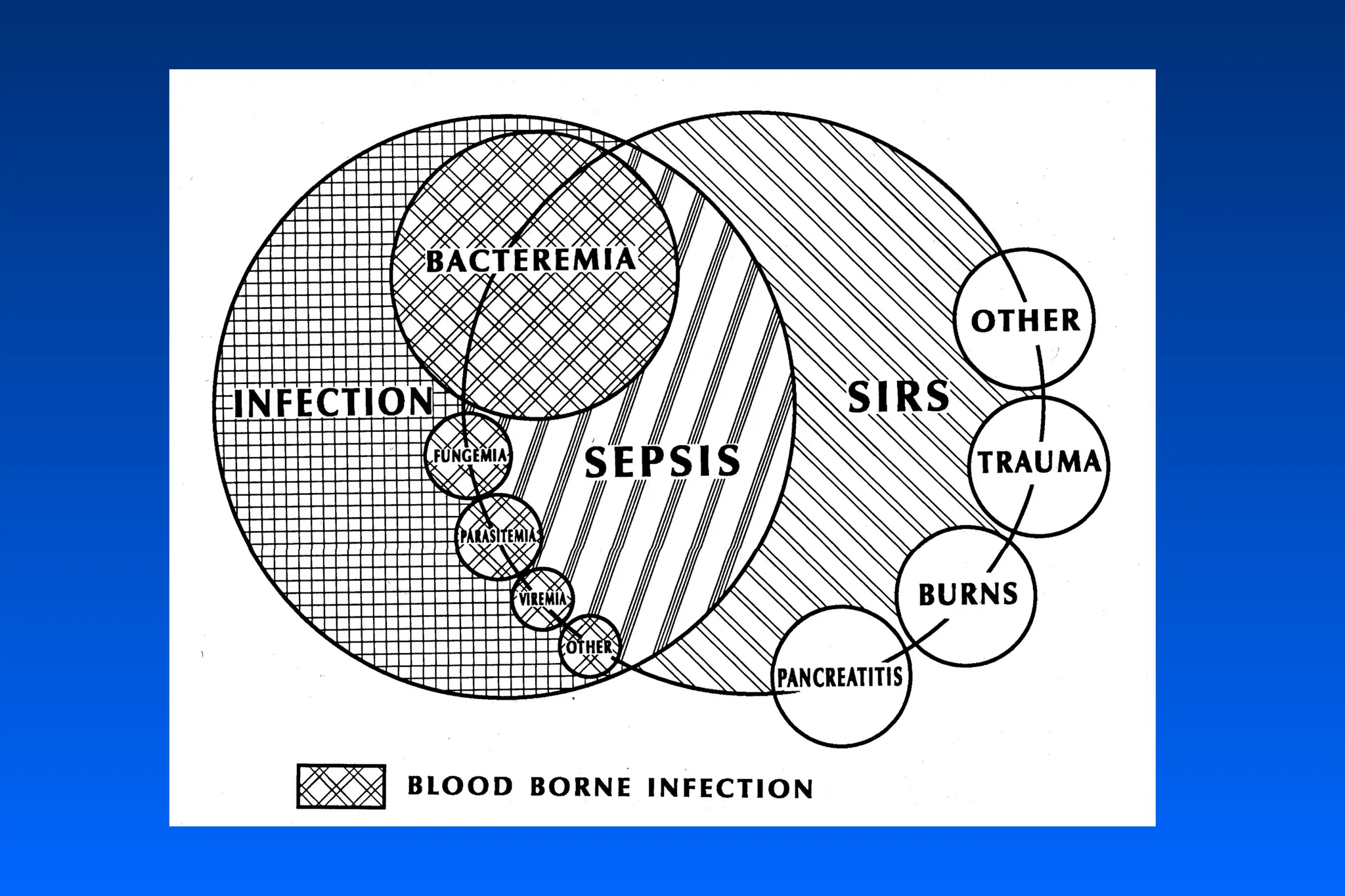
The consensus conference proposed a new term, SIRS, to describe widespread inflammation that occurs following a wide variety of insults including infection, pancreatitis, trauma, burns, etc.
It is agreed that sepsis, severe sepsis and septic shock represent a continuum in a disease process and are correlated with increasing organ dysfunction and mortality.
#4 Angus DC et al.2001. Crit Care Med 29:1303-1310.
Balk RA.2000. Crit Care Clin 16(2):179-191.
#7 Definitions – ACCP/SCCM
Bone et al.1992. Chest 101:1644-1655.
Bands = immature neutrophils
Pro-inflammatory cytokines
Tumor Necrosis Factor (TNF), IL-1, IL-12, Interferon gamma (IFNgamma), and IL-6.
#8 Definitions – ACCP/SCCM
Consensus Conference Definition
Bone et al.1992. Chest 101:1644-1655.
Sepsis: a systemic inflammatory response to infection
Severe Sepsis: systemic inflammation, coagulation and impaired fibinolysis.
Septic Shock: severe sepsis defined as sepsis-induced hypotension (systolic blood pressure < 90mmHg or a reduction of=40mmHg from baseline in the absence of other causes for hypotension) despite adequate fluid resuscitation along with the presence of perfusion abnormalities. Patients receiving inotropic or vasopressor agents may no longer be hypotensive by the time that they manifest hypoperfusion abnormalities or organ dysfunction, yet they would be considered having septic shock.
#9 Definitions – ACCP/SCCM
Bone et al.1992. Chest 101:1644-1655.
The criteria for organ dysfunction are:
• respiratory: PaO2/FiO2=250 without pneumonia and =200 if pneumonia present;
• renal: urine output < 0,5 ml/kg/h;
• hematological dysfunction: platelets count < 80000/mm3; or 50% decrease in platelet count from highest value recorded over previous 3 days;
• metabolic acidosis: pH=7,3 or base deficit =5mEq/l and plasma lactate level >1,5 times the upper limit of normal;13
• cardiovascular: cardiovascular shock (see at the septic shock).
Multiple organ dysfunction syndrome (MODS)
A syndrome in which the hypotension and hypoperfusion, secondary to the pathophysiological alterations in severe sepsis, result in dysfunction in more than one organ or system
#11 Sepsis
A systemic inflammatory response to infection
Severe Sepsis
Sepsis with one or more dysfunctional organs or systems (e.g., cardiovascular dysfunction as indicated by hypotension and shock that is resistant to fluid resuscitation, respiratory dysfunction as indicated by hypoxemia, renal dysfunction as indicated by anuria or oliguria)
Septic Shock
Severe sepsis with hypotension that is resistant to fluid resuscitation and requires pharmacological intervention (vasopressors and/or inotropic agents)
Compensatory anti-inflammatory response syndrome (CARS)
A syndrome in which anti-inflammatory mediator release overcompensates for the systemic inflammatory response to an infectious and/or traumatic insult leading to a state of immune suppression, increased susceptibility of the critically ill patient to infection, and impaired recovery
Multiple organ dysfunction syndrome (MODS)
A syndrome in which the hypotension and hypoperfusion, secondary to the pathophysiological alterations in severe sepsis, result in dysfunction in more than one organ or system
#12 Definitions – ACCP/SCCM
Compensatory anti-inflammatory response syndrome (CARS)
A period of immuno-depression. Persistence of this hypo-responsiveness is associated with increased risk of nosocomial infection and death.
Pro-inflammatory cytokines
Tumor Necrosis Factor (TNF), IL-1, IL-12, Interferon gamma (IFNgamma), and IL-6.
Anti-inflammatory cytokines
(IL-10), soluble inhibitors [TNF receptors, IL-1 receptor type II, and IL-1RA (an inactive form of IL-1)].
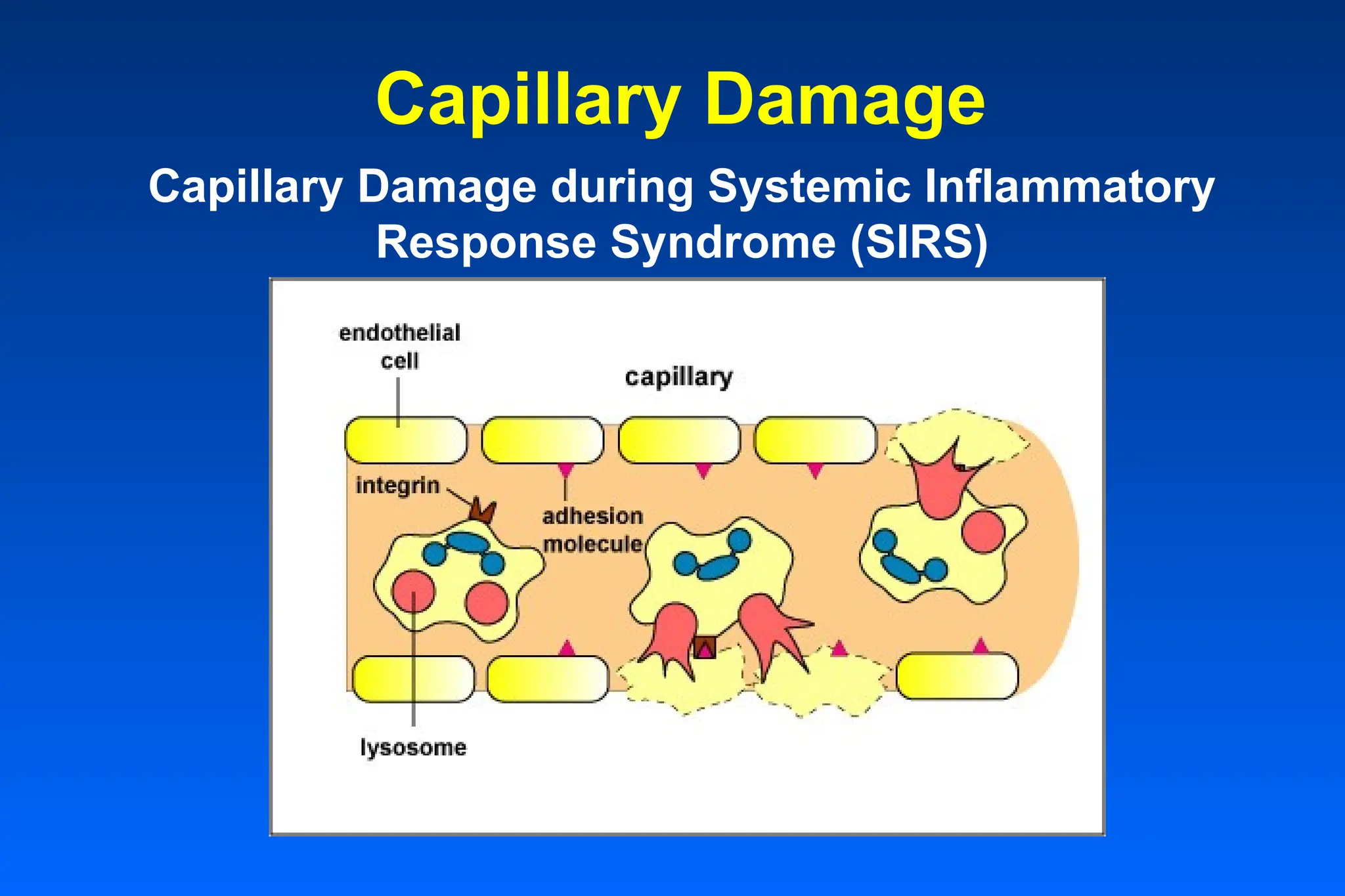
#14 With the production of large amounts of pro-inflammatory cytokines, neutrophils adhere to capillary walls in massive amounts. Chemokines cause neutrophils to release proteases and toxic oxygen radicals, the same chemicals they use to kill microbes, but these toxic chemicals are now being dumped onto the vascular endothelial cells to which the neutrophils have adhered during diapedesis. This results in damage to the capillary walls and leakage of blood.
#15 Chronic Illness: Diabetes mellitus
Immune Deficiency:Transplant recipients and transplantation procedures
Antibiotic Resistance: Increasing number of community-acquired and nosocomial infections
#16 Risk factors
Any condition that compromises the host defense system increases the likelihood of infection and sepsis.
Incidences projected to rise to 1.0 million cases annually in the US within the next decade due to:
Aging population
Increased awareness and diagnosis
Immunocompromised patients
Invasive procedures
Resistant pathogens
#17 In fact what happens is a vicious cycle of inflammation and coagulation, with ischemia, cell damage and finally organ dysfunction and death.
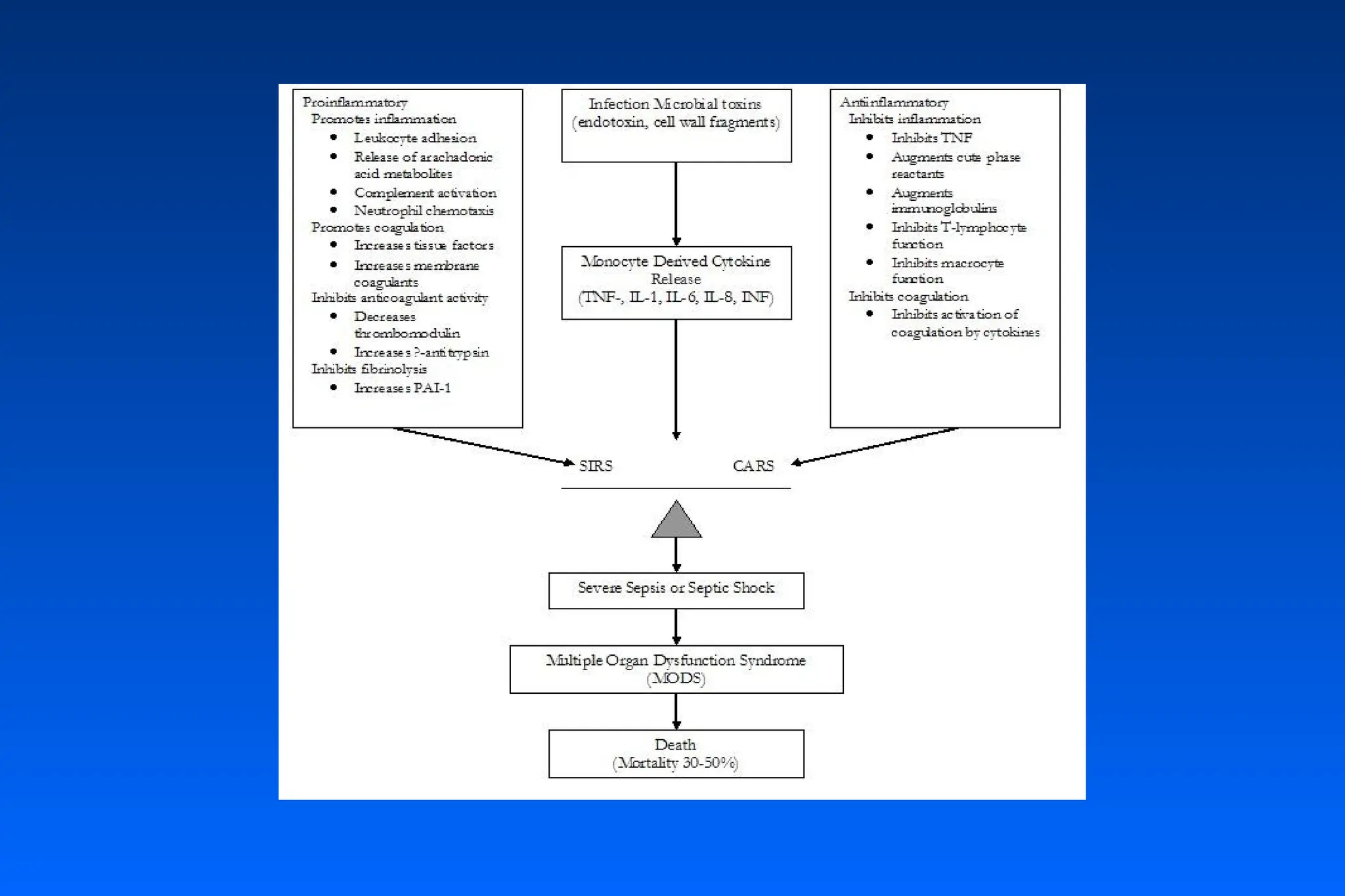
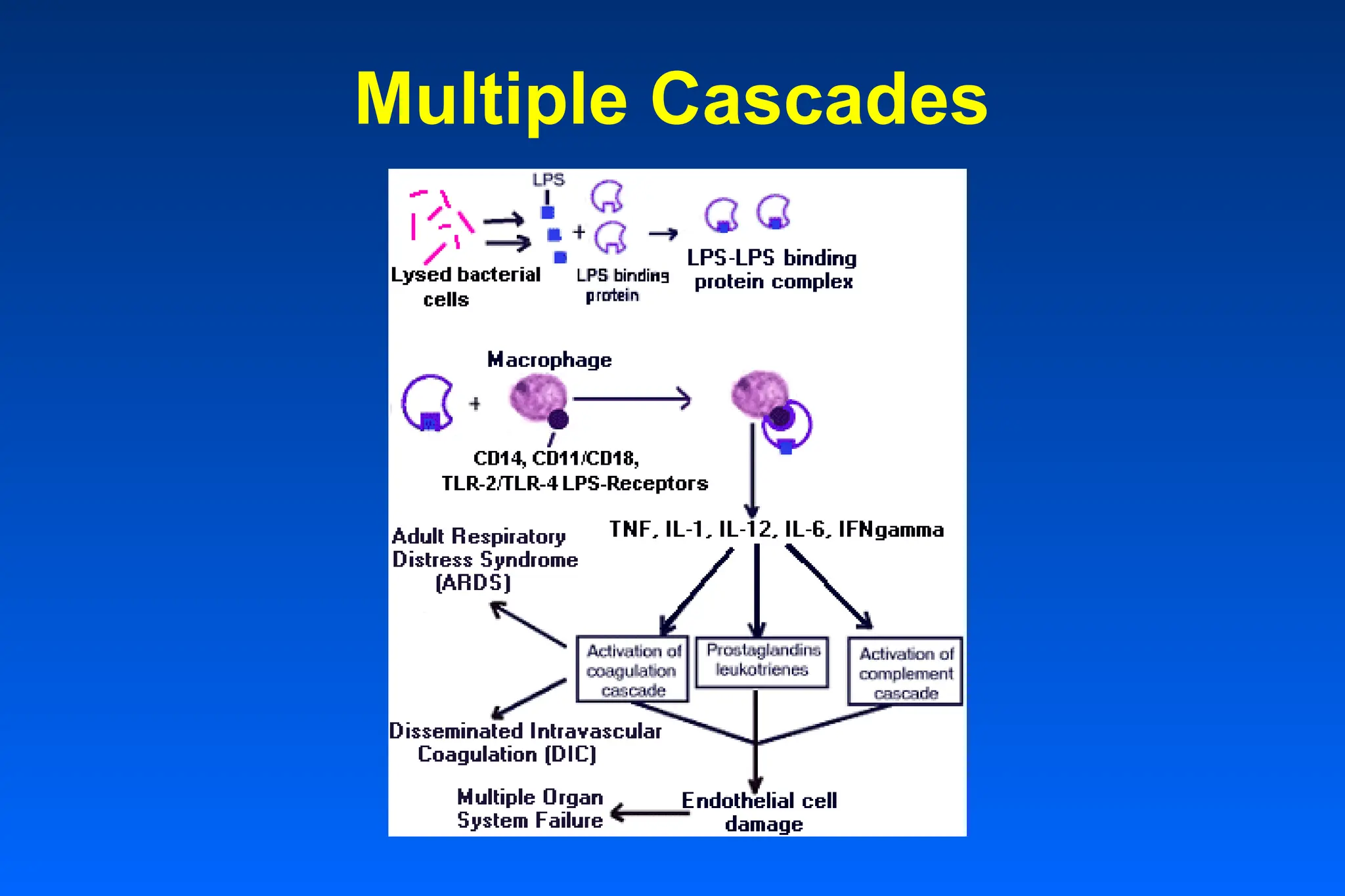
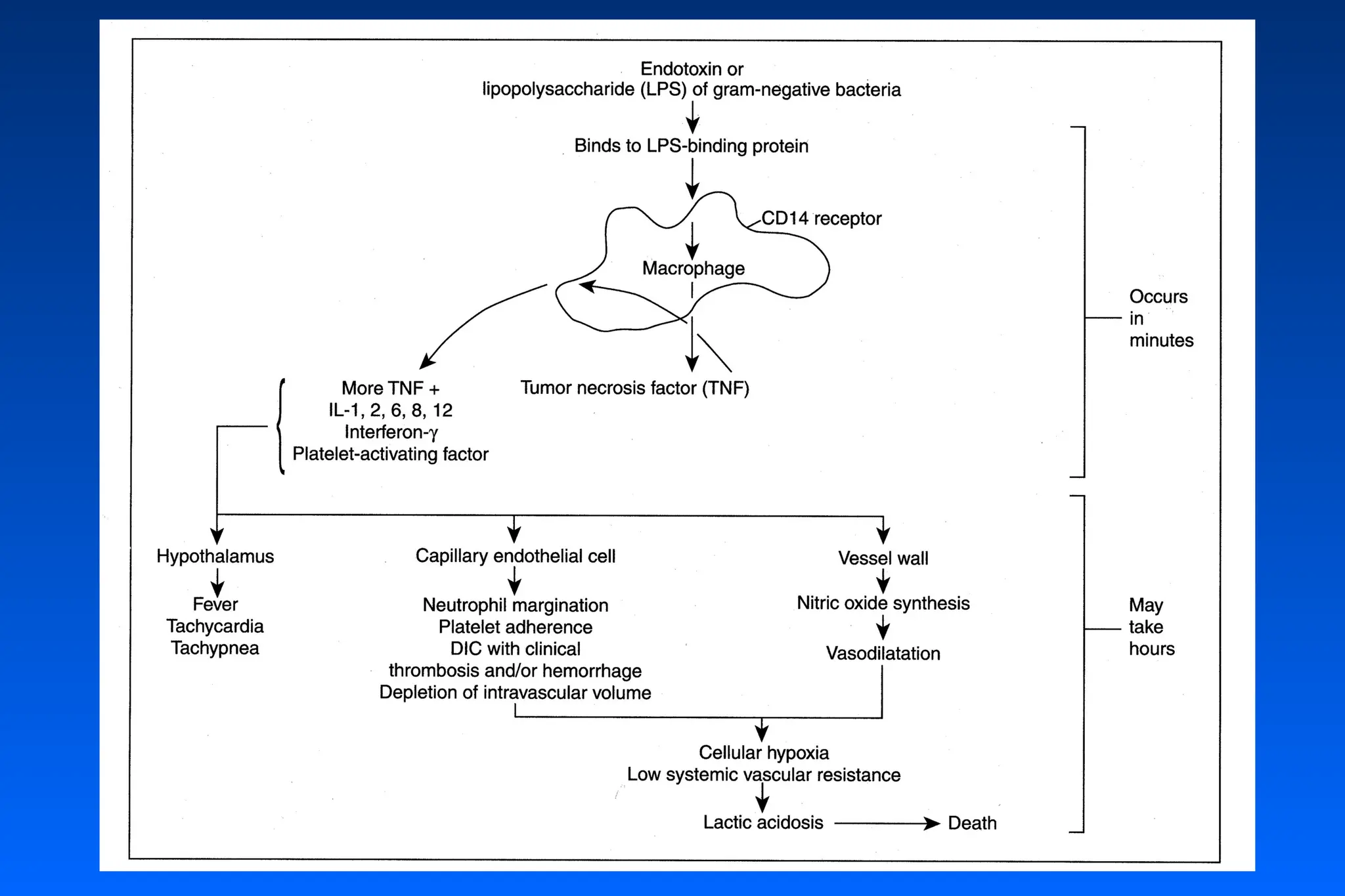
#18 Pro-inflammatory cytokines
Tumor Necrosis Factor (TNF), IL-1, IL-12, Interferon gamma (IFNgamma), and IL-6.
TNF and IL-1 (as well as endotoxins) can also cause the release of tissue-factor by endothelial cells leading to fibrin deposition and DIC.
These mediators cause the activation of the coagulation cascade, the complement cascade and the production of prostaglandins and leukotrienes.
Anti-inflammatory cytokines
(IL-10), soluble inhibitors [TNF receptors, IL-1 receptor type II, and IL-1RA (an inactive form of IL-1)].
Ultimately, hypoperfusion of major organs may occur with the end result being the multiple organ dysfunction syndrome (MODS).
#19 TNF=tumor necrosis factor; IL=interferon; PAI=plasminogen activator inhibitor.
All of the factors can lead to severe sepsis/septic shock/MODS/Death.
#20 Interaction between coagulation system and inflammatory response
The coagulation system and anti-inflammatory cascade work in concert, with one potentiating the effects of the other.
Thrombin not only plays a key role in the coagulation cascade but also has important inflammatory and cellular proliferative properties.
The inflammatory system also has a strong influence on the coagulation system. Endotoxins and the the pro-inflammatory cytokine TNF stimulate coagulation.
These interactions realize a vicious circle of inflammation and coagulation, which leads to organ hypoperfusion, organ failure and finally death.
Clots lodge in the blood vessels which lowers profusion of the organs and can lead to multiple organ system failure. In time this activation of the coagulation cascade depletes the patient's ability to make clot resulting in DIC and ARDS.
#21 Fibrinolysis is impaired.
Thrombin, itself, is an activator of inflammation and inhibitor of fibrinolysis.
#22 The cumulative effect of the cascades is an unbalanced state, with inflammation dominant over anti-inflammation and coagulation dominant over fibrinolysis.
Microvascular thrombosis, hypoperfusion, ischemia, and tissue injury result.
Severe sepsis, shock, and multiple organ dysfunction may occur, leading to death.
#23 Complement system
Bacterial products, including endotoxin, can activate the classical and alternative complement pathways - an important part of the normal host defense mechanism aimed at facilitating bacterial clearance. The complement activation causes an increased release of IL-1, TNF and other inflammatory mediators, thus sustaining the sepsis response. C5a is perhaps one of the most important complement factors in the pathogenesis of sepsis, stimulating the adhesion and degranulation of lymphocytes. Degranulation results in the release of proteases and oxygen-free radicals causing endothelial damage. This sequence is seen particularly in the lung and could be of importance in the pathogenesis of ARDS.
Contact system
The contact system is activated by various factors during sepsis, including endotoxin-stimulated Factor XII. The resultant conversion of prekalikrein to kalikrein and subsequent cleavage of kininogen to release bradikinin has been implicated in septic shock, since bradikinin is a potent vasodilator.
PAF
PAF stimulates G-protein coupled receptors to activate phospholipases. PAF is a potent vasodilator in most vascular beds, but cause vasoconstriction in the pulmonary, renal and coronary beds. In addition, PAF increases vascular permeability and stimulates platelets aggregation and activation with the release of histamine and serotonin. PAF also encourages neutrophil aggregation and degranulation, with the release of leukotrienes and the production of superoxide. It has been implicated in the hypotension and myocardial depression of septic shock, and a recent trial suggests a decreased incidence of organ dysfunction in septic patients treated with PAF antagonist.26
Arachidonic acid metabolites
Arachidonic acid is released from cellular phospholipids and enters either the cyclooxigenase pathway, resulting in the formation of prostaglandins (PG) and thromboxane (Tx), or the lipooxigenase pathway, resulting in the formation of leukotrienes. PGE2 is a vasodilatator and may thus contribute to the hypotension seen in septic shock, but it also inhibits platelet aggregation, and such may have a protective effect on capillary potency. TxA2 causes a vasoconstriction in the pulmonary vasculature and induces platelet aggregation. Leukotriene B4 is a potent chemotactic and activating agent for polymor-phonuclear neutrophils (PMNs) resulting in the production of superoxide.
Reactive oxygen species (ROS)
ROS are produced by various mechanisms during sepsis, including PMN degranulation and eicosanoids metabolism. ROS cause cell membrane damage by degrading lipids and proteins, including DNA. In the erythrocyte, this can result in red cell deformation, encouraging microcirculatory perfusion deficits. In the endothelium ROS-induced increased permeability promotes edema formation.
Nitric oxide (NO)
Nitric oxide (NO) is produced in large amounts during sepsis by stimulation of inducible NO syntethase and clearly has both protective and potentially harmful effects during septic shock. NO has been implicated in the hypotension and myocardial depression in sepsis. NO combines with superoxide to form peroxynitrate, which has toxic effects, including inhibiting mitochondrial respiration.
#27 ●Cardiovascular
● Systemic vasodilation and hypotension (Psys < 90 mmHg)
● Tachycardia (>100 beats/min)
● Increased cardiac output (hyperdynamic), although contractility is depressed; hypodynamic in late shock
● Ventricular dilation; decreased ejection fraction
● Loss of sympathetic responsiveness
● Hypovolemia due to vascular leakage; central venous pressure may be decreased or increased depending upon fluid resuscitation
● Compromised nutrient blood flow to organs; decreased organ oxygen extraction
Pulmonary & Renal
● Hyperventilation with respiratory alkalosis
● Pulmonary hypertension and edema
● Hypoxemia (arterial pO2 < 50 mmHg)
● Reduced pulmonary compliance; increased work
● Respiratory muscle failure
● Renal hypoperfusion; oliguria
● Acute tubular necrosis and renal failure
Other
● Disseminated intravascular coagulation (DIC)
● Blood dyscrasias
– leukopenia
– thrombocytopenia
– polycythemia
● Central and peripheral nervous dysfunction
● Increased lactate occurs early
#33 Organ Dysfunctions associated with Severe Sepsis and Septic Shock:
Lungs: early fall in arterial PO2, Acute Respiratory Distress Syndrome (ARDS): capillary-leakage into alveoli; tachypnea, hyperpnea
Kidneys (acute renal failure): oliguria, anuria, azotemia, proteinuria
Liver- elevated levels of serum bilirubin, alkaline phosphatase, cholestatic jaundice
Digestive tract- nausea, vomiting, diarrhea and ileus
Skin - ecthyma gangrenosum (think Pseudomonas aeruginosa in neutropenic patients), Petechia or purpura (think Neisseria meningitidis or Rickettsia rickettsia (if evidence of tick bite)), Hemorrhage or bullous lesions in patient who has eaten raw oysters (Vibrio vulnificus), generalized erythroderma (Toxic Shock Syndrome= Staphylococcus aureus or Streptococcus pyogenes)
Heart- cardiac output is initially normal or elevated,
Brain - confusion
#34 EARLY SEPSIS; leukocytosis with left shift, thrombocytopenia, hyperbilirubinemia, and proteinuria. Leukopenia may occur. Hyperventilation commonly induces respiratory alkalosis. Hypoxemia correctable with oxygen. Diabetics can develop hyperglycemia. Serum lipids are elevated.
#35 LATER ON: Thrombocytopenia worsens with prolongation of thrombin time, decreased fibrinogen, and presence of D-dimers suggesting DIC. Azotemia, and hyperbilirubinemia are more prominent. Liver enzymes become elevated. When respiratory muscles fatigue the accumulation of serum lactate occurs. Metabolic acidosis (increased anion gap) supervenes the respiratory alkalosis. Hypoxemia not correctable even with 100% oxygen. Diabetic hyperglycemia can precipitate ketoacidosis worsening the hypotension.
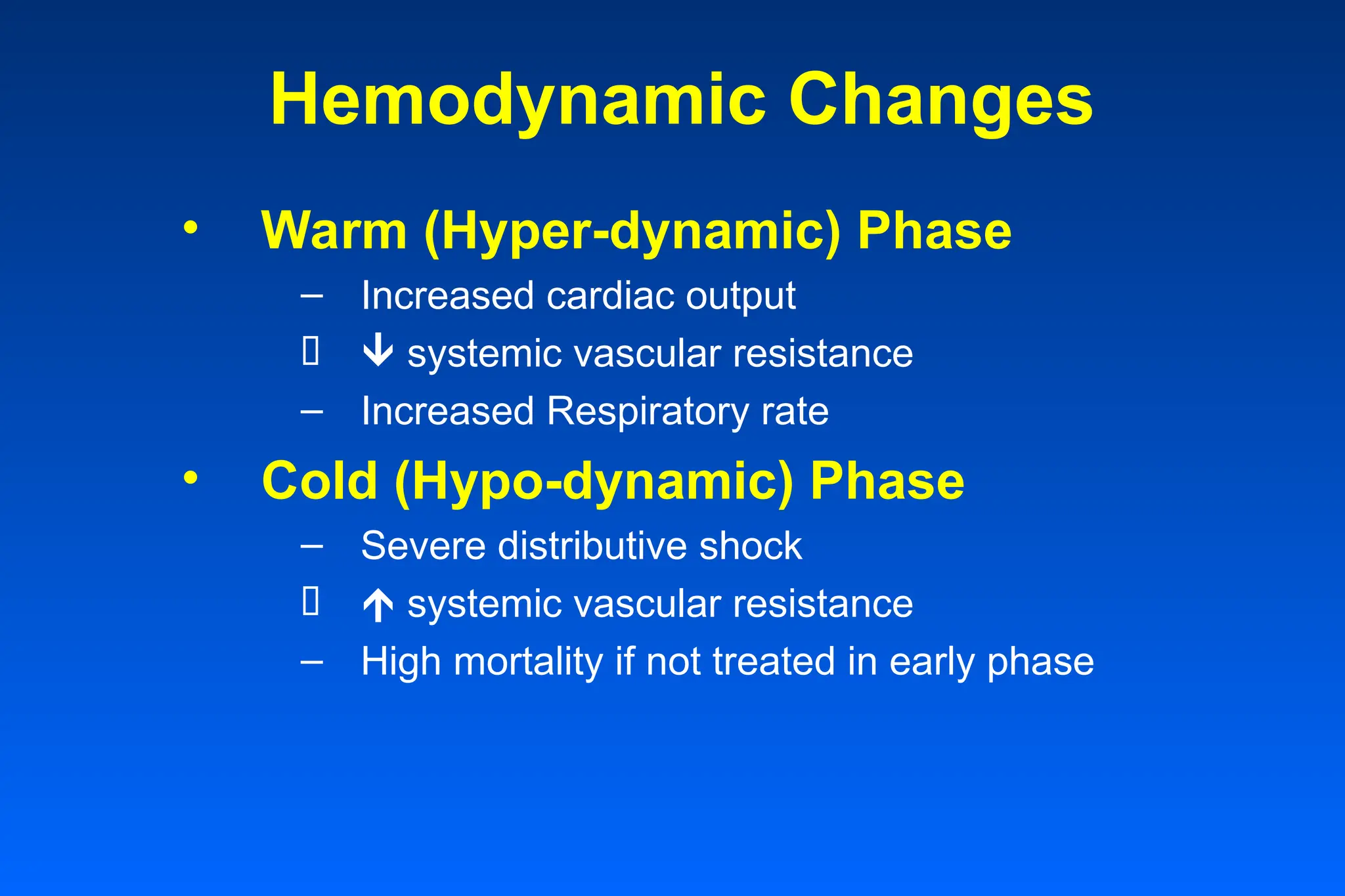
#38 Warm (Hyper-dynamic) Phase
Increased cardiac output
Due to endotoxin effects (in spite of myocardial depressant effect)
systemic vascular resistance
Due to increased vascular permeability
Fluids shift
Increased Respiratory rate
Due to endotoxin stimulation of medulla
Cold (Hypo-dynamic) Phase
Severe distributive shock
Hypovolemic shock
Fluid volume in tissues
systemic vascular resistance
Endotoxin effects wear off
Compensatory shock effort
High mortality if not treated in early phase
#40 Adult respiratory distress syndrome (ARDS)
Disseminated Intravascular Coagulation (DIC)
Acute Renal failure (ARF)
Intestinal bleeding
Liver failure
Central Nervous system dysfunction
Heart failure
Death
#41 Optimize intravascular volume
Consider Xygris (Activated Protein C)
#45 The main effect of protein C is to reduce the production of thrombin
Protein C has profibrinolytic properties
Anti-inflammatory effects
– Inhibits cytokine production & release
– Inhibits neutrophil activation & endothelial damage
Anticoagulant effects
– Ultimately limits generation of thrombin
Fibrinolysis effects
– Inactivates PAI-1 to promote homeostatic thrombolysis by tPA
– Inhibits TAFI activation to maintain fibrinolysis
#46 Xigris has a short half-life, indicating rapid inactivation of Xigris after stopping infusion.
Approximately 80% of Xigris is eliminated within 30 minutes.
Xigris should be discontinued 2 hours prior to performing an invasive surgical procedure or procedures with an inherent risk of bleeding.
Initiation of Xigris once hemostasis has been achieved:
May restart immediately after uncomplicated, less invasive procedures.
Reconsider 12 hours after major invasive procedures or surgery.
3.Immediately stop the administration of Xigris if clinically important bleeding occurs.
4.There is no evidence that Xigris therapy requires that routine laboratory tests or hemostatic parameters be monitored.
#47 Dosing and administration
The following information is important in determining dosage and administration of Xigris:
Xigris should be administered intravenously at a continuous infusion rate of 24 µg/kg/hr for a total duration of infusion of 96 hours.
Each IV administration should be completed within 14 hours after preparation of the solution.
Dosage calculation should be based on patient's actual body weight at start of Xigris treatment, and should remain constant regardless of weight fluctuations.
No titration is necessary. Bolus dosing or dose escalation is not recommended.
Xigris should be administered via a dedicated intravenous line or a dedicated lumen of a multilumen central venous catheter.
If the infusion is interrupted, Xigris should be restarted at the initial infusion rate and continued to complete the recommended duration of infusion.
Xigris is available in 5-mg and 20-mg single-use vials containing sterile, preservative-free, lyophilized drotrecogin alfa (activated).
Contraindications
Xigris is contraindicated in patients with the following clinical situations:
Active internal bleeding
Recent—within 3 months—hemorrhagic stroke
Recent—within 2 months—intracranial or intraspinal surgery, or severe head trauma
Trauma with increased risk of life-threatening bleeding
Presence of an epidural catheter
Intracranial neoplasm or mass lesion or evidence of cerebral herniation
Known hypersensitivity to drotrecogin alfa (activated) or any component of this product
#51 CHEST 2001;120:989-1002.
New Engl J Med 2001;345:588-595.
#53 We cannot know what is next on our horizon.
We have only just begun to understand some of the complexities of the human body.
We have so much further to go.
#54 American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med 1992;20:864-74.
Anderson RN. Deaths: Leading causes for 1999. National vital statistics reports; vol 49 no 11. Hyattsville, Maryland: National Center for Health Statistics. 2001.
Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 2001;29:1303-10.
Fish DN. Optimal antimicrobial therapy for sepsis. Am J Health-Syst Pharm 2002;59(suppl 1):S13-19.
Bone RC, Grodzin CJ, Balk RA. Sepsis: a new hypothesis for pathogenesis of the disease process. Chest 1997;112:235-43.
Rangel-Frausto MS, Pittet D, Costigan M, et al. The natural history of the systemic inflammatory response syndrome (SIRS): a prospective study. JAMA 1995;272:117-23.
Vervloet MG, Thijs LG, Hack CE. Derangements of coagulation and fibrinolysis in critically ill patients with sepsis and septic shock. Semin Thromb Hemost 1998;24:33-44.
Kuhl DA. Current strategies for managing the patient with sepsis. Am J Health-Syst Pharm 2002;59(suppl 1):S9-13.
Esmon CT. Inflammation and thrombosis: mutual regulation by protein C. Immunologist 1998;6:84-9.
Grey ST, Tsuchida A, Hau H, et al. Selective inhibitory effects of the anticoagulant activated protein C on the responses of human mononuclear phagocytes to LPS, IFN-gamma, or phorbol ester. J Immunol 1994;153:3664-72.
Bernard GR, Vincent J, Laterre P, et al. Efficacy and safety of recombinant human activated protein C for severe sepsis. N Engl J Med 2001;344:699-709.
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med 1985;13:818-29.
Drotrecogin alfa (activated) (Xigris), Eli Lilly and Company, 2001 (prescribing information).



































![Understanding Parkinson’s Disease: Causes, Symptoms, and Treatment [2025]](https://cdn.slidesharecdn.com/ss_thumbnails/understandingparkinson-251208102525-80ba3223-thumbnail.jpg?width=640&height=640&fit=bounds)














