THE SENSORY INTEGRATION APPROACH OCCUPATIONAL THERAPY
1.
AYRES SENSORY INTEGRATIONFRAME OF
REFERENCE
PRESENTED BY
M.A MUHAMMAD EASA
MOT 1ST
YEAR (NEUROLOGY)
SRFOT
SRIHER
2.
SENSORY INTEGRATION
TheSensory Integration frame of reference was developed by A. Jean
Ayres, an Occupational Therapist with postdoctoral training in
education psychology and neuroscience.
The theory of Sensory Integration postulates that
“Adequate processing and integration of sensory information is an
important foundation for adaptive behavior.”
THEORETICAL BASE FORSI
The theory of sensory integration combines concepts from human development,
neuroscience, psychology, and occupational therapy into a holistic framework for
viewing behavior and learning.
Accordingly, there are seven basic theoretical postulates that form the foundation for
the sensory integration frame of reference.
1. Sensory information provides an important foundation for learning and behavior.
2. Sensory integration is a developmental process.
3. Successful integration and organization of sensory information results in and is
further developed by adaptive responses.
5.
4. The‘‘just right challenge’’ provides the milieu for sensory integration to occur.
5. Children have an innate drive to seek meaningful experiences from their
environment.
6. As a result of neuroplasticity, enriched experiences effect change in the nervous
system.
7. Sensory integration is a foundation for physical and social engagement and
participation in daily life activities and routines.
6.
The sensory integrationframe of reference focuses on the
• TACTILE
• VESTIBULAR
• PROPRIOCEPTIVE SENSATIONS
To create ‘‘body maps’’ that are used to guide movement and motor
planning.
7.
HOW DO CHILDRENLEARN ?
“Through exploration with their senses”
8.
KEY SENSORY INTEGRATIVEABILITIES
The abilities supported by sensory integration are consistent with the patterns
of function and dysfunction identified through research. They include
Sensory modulation,
Sensory discrimination (primarily tactile, vestibular, and proprioceptive as
well as auditory, visual, taste, and smell),
Postural-ocular control,
Praxis, and
Bilateral integration and sequencing.
9.
SENSORY MODULATION
Sensorymodulation refers to an individual’s ability to respond adaptively to
sensation over a broad range of intensity and duration (Lane, 2002 ).
Sensory modulation provides the foundation to perform adaptively in day-to-
day occupations.
Children with adequate sensory modulation are able to tolerate various
sensations offered in the environment
10.
SENSORY DISCRIMINATION
Theability to discriminate sensory information allows the development of
perceptions of events and self in action and contributes to skill development, learning,
social interactions, and play that especially involves fine, discrete responses such as
object manipulation.
Somatosensory discrimination
Proprioceptive discrimination
Discrimination of vestibular.
POSTURAL-OCULAR CONTROL
Postural-ocularcontrol involves activating and coordinating muscles in response to
the position of the body relative to gravity and sustaining functional positions
during transitions and while moving.
Postural control is dependent not only on adequate muscle tone, coactivation of
muscles, and ability to activate muscle synergies but also on adequate ability to
integrate sensory information from the vestibular, proprioceptive, visual, and tactile
systems.
Balance and equilibrium are components of postural control that are modulated by
the vestibular, proprioceptive, and visual systems. Daily activities require
coordinating the position of the body relative to gravity by organizing not only
upright postures but also the coordination of the two sides of the body.
13.
PRAXIS
Praxis isthe ability to plan and organize a sequence of goal-directed motor actions.
Praxis is developed through meaningful and successful motor interactions with the
world. Repetition of successful actions encodes the action in a motor engram or
‘‘neural map’’ in our nervous system.
Ayres (1985) felt that praxis involves cognition as well as planning and motor skills.
14.
Praxis is developedthrough
meaningful and successful
motor interactions with the
world.
16.
FUNCTION–DYSFUNCTION CONTINUA FORTHE SENSORY
INTEGRATION FRAME OF REFERENCE
The theoretical base of a frame of reference delineates those problems with which the frame of reference is concerned.
Behaviors are examined within the context of the function–dysfunction continua to determine the need for
intervention. A cluster of behaviors is necessary to be identified as requiring intervention using a sensory integrative
approach.
• This means therapists observe behaviors on a spectrum from typical function to dysfunction.
• Example: A child who occasionally avoids loud noises (functional) vs. a child who cannot tolerate any sound and
hides or screams (dysfunctional).
Atypical responses (i.e., unusual over-, under-, or fluctuating responsivity) to the sensory aspect of materials,
activities, or situations (sensory modulation disorder).
Poor ability to conceptualize, plan, and execute motor actions associated with signs of poor perception of touch and
body position (somatodyspraxia).
Poor ability to coordinate both sides of the body, and atypical postural and ocular mechanisms associated with signs of
inefficient processing and perception of movement and body position (bilateral integration and sequencing deficit).
Poor visual perception and visual motor integration (constructional and visuo dyspraxia).
17.
SENSORY MODULATION ABILITIES
Sensory modulation describes the way in which an individual responds to sensory
stimuli in the environment.
Proposed are three subtypes of sensory modulation disorder:
Over-responsivity
Under-responsivity
Sensory seeking
18.
SENSORY OVER-RESPONSIVITY
Sensoryover-responsivity is characterized by an excessive or exaggerated response
to sensory stimuli that are not perceived as threatening, harmful, or noxious by
typically developing children.
The fight, flight, or freeze reactions manifested by individuals who are over-
responsive can produce anxiety, hyperactivity, and inattention.
19.
TACTILE
• Difficulty withgetting haircuts
• Avoidance of touching certain textures
• May dislike certain foods because of texture
• May dislike brushing teeth, using toothpaste
• Responds with alarm or withdrawal when the face is wiped
• Has an aversion to haircuts, combing, washing, and showering
• Avoids walking or crawling on surfaces such as rugs or grass
• Prefers to wear clothing that covers his/her body, regardless of temperature; may prefer
no clothing at all
• Does not like the feel of certain clothing, tags, sheets
•
SENSORY OVER-RESPONSIVITY
20.
VESTIBULAR
• Disoriented afterbending down
• Anxious when feet leave the ground
• Avoids rapid or rotating movements
• Gets car sick, dislikes carnival rides
• Is scared to jump, go up or down stairs, roll in a barrel, climb, lean over
backward to wash hair, do somersaults, rough-house, swing
• Gravitational insecurity
• Postural insecurity
VISUAL
• Difficulty tolerating bright lights
SENSORY OVER-RESPONSIVITY
21.
PROPRIOCEPTION
• Difficulty beinghugged
• Difficulty with people moving your body
• Clumsiness
• Tendency to fall
• Lack of awareness of body position in space
• Odd body posturing, minimal crawling when young
• Difficulty manipulating small objects (buttons, snaps)
• Eating in a sloppy manner
• Resistance to new motor movement activities
SENSORY OVER-RESPONSIVITY
22.
ORAL
• “Picky” eater
•Difficulty brushing teeth
AUDITORY
• Fearful of sounds
• Distracted by certain noises
• Frequently cover ears
SENSORY OVER-RESPONSIVITY
23.
SENSORY UNDER-RESPONSIVITY
Sensoryunder-responsivity describes children who exhibit less response to sensory
information than the situation demands, taking longer time to react or requiring a
higher intensity/longer duration of sensory messages before they are moved to
action.
Children with under-responsivity may exhibit passive behavior. Children who do not
detect, register, or notice sensation in the environment do not have a drive to interact
or to engage in occupation.
24.
TACTILE
• Difficulty noticingtouch
• Dress inappropriately for weather
• Does not react to painful experiences
• has difficulty manipulating tools and toys
VISUAL
• Often miss what is right in front of them
SENSORY UNDER-RESPONSIVITY
25.
VESTIBULAR
• Is clumsy,stumbles, falls
• Bilateral integration, lacks hand dominance, cross midline
• confuses right and left
• Reverses letters and reads words backwards
• Has delays in speech, reading, and writing as well as in visual perception
• Can not follow a moving object, draw a line, read a line of print easily, or copy from
the board
• Has trouble holding his or her head up while sitting; may tire easily not get dizzy,
loves fast-moving equipment
• Enjoys being upside down or sideways
SENSORY UNDER-RESPONSIVITY
26.
PROPRIOCEPTION
• Poor bodyawareness
• Floppy or poor posture
• Constantly jumping,
• Crashing
• stomping
• loves to be squished and bear hugs
• prefers tight clothing
• loves rough-housing
• may be aggressive with other children.
SENSORY UNDER-RESPONSIVITY
27.
AUDITORY
• Listens toloud music or TV
• Talks to self during a task (out loud)
ORAL
• May be able to eat anything
SENSORY UNDER-RESPONSIVITY
28.
SENSORY SEEKING
Sensoryseeking describes children who actively look for or crave sensory
stimulation and seem to have an almost insatiable desire for sensory input.
Sensory seeking children are overly active, constantly moving, touching, watching
moving objects, and/or seeking loud sounds or intense olfactory or gustatory
experiences.
They may engage in risky behaviors such as climbing and jumping from playground
equipment that is not designed for this activity as well as excessive spinning,
mouthing of objects, touching things, or making noises.
29.
Tactile
• Enjoy “bear”hugs
• Crave touch of textures
Vestibular
• Jumping
• Enjoy spinning in circles, being upside down
Proprioception
• Loves crashing or bumping into objects
• Craves highly physical activities
Auditory
• Speaks louder than necessary
• Needs to listen to music to concentrate
Oral
• Puts anything in the mouth (searching for oral input)
30.
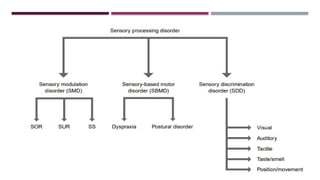
SENSORY DISCRIMINATION DISORDER
PROPRIOCEPTION
•Constant slamming of doors
• Pushing too hard (to increase awareness)
TACTILE
• Need to use eyes when searching for object in backpack or purse
TASTE/SMELL
• Difficulty distinguishing between flavors or scents
VESTIBULAR
• Frequently falls out of chairs
31.
SENSORY BASED MOTORDISORDER
Dyspraxia - Difficulty motor planning
Postural disorder
• Poor co-contraction
• Muscle tone (Low)
• Equilibrium and posture
• Immature reflexive abilities
• Bilateral Integration
32.
DYSPRAXIA
Somatodyspraxia isdescribed as a deficit in learning new motor skills, planning new
motor actions, and generalizing motor plans.
When motor planning abilities are not working well, the child struggles to complete
new or complex motor tasks.
Somatodyspraxia is the most common form of dyspraxia seen in children with sensory
integrative disorder and is closely related to deficits in somatosensory processing.
Ideation:
Ideation is the conceptualization of a goal and some idea of the steps necessary to
achieve that goal. Children who have difficulty with ideation do not recognize play
opportunities with novel toys so they tend to act on all toys with a limited set of
behaviors such as lining up, throwing, swinging, or breaking.
33.
• Poor grossmotor skills
• Running
• jumping
• Poor fine motor skills
• Zipping
• Buttoning
• Problems in figuring out how to do movements
• Dressing
• Complex dance steps
• Proprioception
• Poor motor control and body awareness during dressing
• Vision
• Navigating through crowded hallways
EXAMPLES OF DYSPRAXIA
34.
EXAMPLES OF POSTURALDISORDERS
• Low muscle tone
• ‘Slumped’ in chair
• Leans on things
• Poor balance
• Often trips or bumps into objects
• Difficulty with riding a bike or jumping
• Poor stability
• Sits in awkward positions
• Head and eye stability
• Difficulty when reaching for objects
• Use of two sides of the body
• Not stabilizing paper to write
35.
MOTOR PLANNING
Motorplanning is the ability to automatically organize a motor act so that it can be
performed or implemented. This involves the internal process of organizing one’s
motor actions, without consciously planning out the action.
36.
BILATERAL INTEGRATION ANDSEQUENCING
DYSFUNCTION
Bilateral integration and sequencing dysfunction include deficits coordinating two
sides of the body effectively and difficulty sequencing.
When working well, bilateral integration is readily observable in children’s ability
to smoothly and skillfully complete developmental activities that require the use of
the two sides of the body together in a coordinated fashion such as jumping,
hopping, skipping, riding a bike, or using two hands together to accomplish a task
such as cutting with scissors.
Children with bilateral integration have difficulty coordinating two parts of the
body for bimanual tasks such as holding paper to write or using a knife and fork.
37.
VISUAL PERCEPTION
Visualperception is critical to many of the abilities described earlier and is a
common deficit addressed by the sensory integration frame of reference.
Vision is particularly relevant to our ability to maintain upright postures, to learn
about objects, and to provide us with information about the position of our body in
space.
Visual perceptual abilities are an important component of many cognitive skills that
relate to success in school, finding one’s way in the environment, and performing
simple dressing tasks such as finding one’s clothes in a drawer or the closet
38.
CONSIDERATIONS FOR INTERVENTION
The sensory integration frame of reference is most frequently utilized by occupational
therapists as part of a total program of occupational therapy. The intervention is unique
in that it addresses the underlying sensory-motor substrates of dysfunction rather than
just the functional difficulties itself.
This frame of reference provides opportunities for engagement in sensory motor
activities rich in tactile, vestibular, and proprioceptive sensations. The therapeutic
environment is designed to tap into the child’s inner drive to play.
The therapist observes the child’s responses during the activity and increases or
decreases the sensory and motor demands to create a challenging and therapeutic
environment.
39.
CONT,.
. Thechild experiences joy despite effort and work, which supports the child’s
continued and necessary active participation. These play experiences maintain
motivation and facilitate praxis.
Additionally, this allows the child to develop play skills and to encourage
participation in play.
The therapist–child relationship is a critical component of a sensory integration frame
of reference. This therapeutic relationship must be strong to support the child to
engage in challenging activities.
40.
THE PHYSICAL ENVIRONMENTOF INTERVENTION
The physical environment needs to have adequate space to allow for the flow of
vigorous activity. The arrangement of the equipment and materials needs to be
flexible enough to allow for rapid changes in configuration during an intervention
session. There should be several ceiling hooks with adequate spacing to suspend
hanging equipment.
As with all therapeutic interventions, safety must be maintained at all times in the
therapy environment. This is ensured though the use of mats, cushions, and pillows
that are used to pad the floor underneath all suspended equipment. Equipment
should be adjustable to the size of the child. All equipment must be routinely
checked for safety. Therapists should take great care in self-monitoring their safe
use of equipment
41.
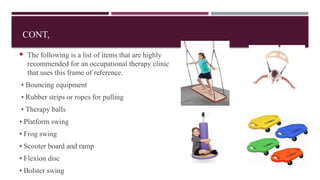
CONT,
The followingis a list of items that are highly
recommended for an occupational therapy clinic
that uses this frame of reference.
• Bouncing equipment
• Rubber strips or ropes for pulling
• Therapy balls
• Platform swing
• Frog swing
• Scooter board and ramp
• Flexion disc
• Bolster swing
42.
EVALUATION
• Sensory History
•Informal observation
• Clinical Observation
• Responses to sensory input
• Praxis
• Checklists
Sensory profile(Winnie and Dunn)
• Sensory integration inventory
• Sensory processing measure(SPM)
• Sensory Integration Praxis Test
• The Gravitational Insecurity Assessment
• The Test of Ideational Praxis
• The Sensory Processing Measure-School
43.
STANDARDIZED SCALES
• SIPT
•The SIPT is a group of 17 tests that are considered the gold standard for diagnosing sensory processing
conditions in children ages 4 to 8 years and 11 months. In addition to tactile, vestibular, and
proprioceptive testing, the SIPT also includes tests related to praxis, coordination, perception.
• MAP
• The MAP is a shorter, easier alternative to the SIPT that can be used to assess sensory challenges in
preschoolers. Like the SIPT, the MAP tests for tactile, vestibular, and proprioceptive challenges, as
well as other learning delays that may be causing difficulties completing classroom tasks.
• Test of sensory function in infants
• Movement assessment battery
• De Gangi Berk Test of SI
1. Sensory inputcan be used systematically to elicit an adaptive response.
2. Registration of meaningful sensory input is necessary before an adaptive response can
be made.
3. An adaptive response contributes to the development of sensory integration.
4. Organization of adaptive responses enhances the child’s general behavioral.
5. More mature and complex patterns of behaviour emerge from the consolidation of
simpler behaviours.
6. The more inner-directed a child’s activities are, the greater the potential for the
activities to improve neural organization
Basic Assumptions Underlying Ayres Sensory Integration Intervention
46.
LEARNING OBJECTIVES
AyresSensory Integration ® Fidelity Measure (ASIFM)
STEP-SI
A SECRET
The physical environment of the intervention
Qualities affecting the intensities of sensations
Therapeutic interventions related to modulation, sensory discrimination,
bilateral integration and sequencing and praxis
Sensory Integration Therapy In ASD, ADHD
47.
In thisintervention, the Occupational Therapist presents activity challenges that are
individually tailored to improve sensory integration capacities of the child.
Ultimately, this intervention is designed to help a child gain competencies and
confidence in performing everyday occupations at home, in play, at school, or in the
community.
48.
ASI interventionis applied on an individual basis because the therapist must adjust
therapeutic activities moment by moment in relation to the individual child’s interest in
the activity or response to a specific challenge or sensory experience
The occupational therapist’s job is to create an environment that evokes increasingly
complex adaptive responses from the child.
Occupational therapy using ASI intervention capitalizes on the inner drive of the child
during intervention.
49.
Active participationis also emphasized because the brain responds di erently and
ff
learns more e ectively when an individual is actively involved in a task, rather than
ff
merely receiving passive stimulation.
Maximal active involvement generally takes place when therapeutic activities are at just
the right level of complexity, at which the child not only feels comfortable and non
threatened but also experiences some challenge that requires e ort. The course of
ff
therapy usually begins with activities with which the child feels comfortable and
competent and then moves toward increasing challenges.
50.
Occupational therapyaims to improve a child’s health and quality of life through engagement in
meaningful and important occupations or activities.
Based on the premise of neuroplasticity in the young and developing brain, sensory integration theory
holds that many of the child’s sensory integration functions improve with individually tailored
therapeutic activities that provide opportunities for exploration and challenge.
In addition to addressing the underlying sensory integration problems, occupational therapists also
often help the child develop specific skills and strategies to minimize the e ects of the problems the
ff
child is experiencing and help the child cope with the current day-to-day demands.
Finally, consulting with parents and teachers to allow for carryover of direct intervention and to plan
modifications of activities, routines, and environments is an important component of any intervention
program involving children.
Parham and colleaguesidentified the key elements of ASI intervention, that is process elements of ASIFM.
10 PROCESS ELEMENTS / Intervention Principles of ASIFM
1. Therapist ensures physical safety of child.
The therapist anticipates physical hazards and attempts to ensure that the child is safe,
and feels physically and emotionally safe, through manipulation of protective and
therapeutic equipment or the therapist ’ s physical proximity and actions.
2. Therapist presents sensory opportunities to the child.
The therapist presents the child with at least two of the following three types of sensory
opportunities: tactile, vestibular, and proprioceptive; the therapist ’ s intent is to use
sensory input to support the development of self-regulation, sensory awareness, or
movement in space. The therapist may provide a variety of sensory opportunities with
varying intensities, qualities, speed, and duration to improve perception, challenge
postural control or praxis, or to attain an adequate arousal state for sustained engagement
53.
3. Therapist supportssensory modulation for attaining and maintaining a regulated state.
The therapist modifies sensory conditions as well as activity challenges and supports to help the
child attain and maintain appropriate levels of arousal and alertness, as well as an affective state and
activity level that supports engagement in activities.
4. Therapist challenges postural, ocular, oral, or bilateral motor control.
Challenges are embedded in sensory-motor activities that build bilateral integration, strength,
dexterity, speed, and agility in static and dynamic postural control, and in fi ne motor, gross motor,
and oral motor skills.
5. Therapist challenges praxis and organization of behavior.
Challenges may address the child ’ s ideation (ability to conceptualize and plan novel movement
activities), motor planning (ability to plan a novel sequence of movements to engage effectively in a
new activity), or organization of behavior in blocks of proximal or distal time and space (e.g.,
planning activities to do in today ’ s session, or next week).
54.
6. Therapist collaborateswith child in activity choice.
The therapist negotiates activity choices with the child, allowing the child to choose
equipment, materials, or specific aspects of an activity. Activity choices and sequences are not
determined solely by the therapist. Instead, the therapist provides structuring and support while
maximizing the child ’ s active control.
7. Therapist tailors the activity to present a just right challenge.
The therapist presents or facilitates challenges that are not too difficult or too easy for the child
to achieve. This may involve altering an activity so that it is easier (more attainable) or more
difficult (requiring more effort). Challenges require some degree of effort and may address
motor control, bilateral coordination, sensory modulation, self-regulation, discrimination and
perception, or praxis and organization of behavior.
55.
8. Therapistensures that activities are successful.
Ensuring success means that the therapist supports the child ’ s experience of success in
doing part or all of an activity. For example, this may be done by altering the task at any
point in the activity sequence, by coaching the child on alternative ways to do the activity,
or by prompting the child to find another strategy.
9. Therapist supports child ’ s intrinsic motivation to play.
This is done by creating a setting that supports play as a way to fully engage in
intervention activities. The therapist builds upon the child ’ s intrinsic motivation and
enjoyment of activities through strategies such as communicating nonverbally or verbally
that play is encouraged, allowing the child to explore or experiment with actions or
objects, or engaging with the child in motor, object, pretend, or social role-play.
56.
10. Therapist establishesa therapeutic alliance with the child.
The therapist promotes and establishes a connection with the child that conveys they are
working together in a mutually enjoyable partnership. Overall, there is a climate of trust,
emotional safety, connectedness, and appreciation of the child.
57.
THE STEP-SI
ByLucy J. Miller, PhD, OTR/L, FAOTA
The STEP-SI ( Miller, Wilbarger, Stackhouse, & Trunnell, 2002 ) is another resource
for making SI theory accessible for direct intervention
STEP-SI, serves as a prompt for remembering the active components (dimensions) of
treatment: Sensation, Task, Environment, Predictability, Self-monitoring, and
Interaction ( Miller et al., 2002 ).
The therapist manipulates each of the STEP-SI dimensions to support or challenge a
child’s developmental capacities, serving to develop capacities or skills in identified
problem areas. The appropriateness of the child’s adaptive response becomes a monitor
that guides the modification of intervention.
58.
The componentsor dimensions of the STEP-SI intervention model comprise these
variables:
S Sensation: Sensory modalities: tactile, vestibular, proprioception, audition, vision,
taste, olfaction, oral input, and respiration. Qualities of sensation: duration, intensity,
frequency, complexity, and rhythmicity.
T Task: Structure, complexity, demand for skill, demand for sustained attention, level of
engagement, fun, motivation, and purposefulness (based on standard task analysis)
E Environment: Organization, complexity, perceived comfort and safety, and
possibilities for engagement, exploration, expansion, and self-challenge
59.
P Predictability:Novelty, expectation, structure, routine, transitions, and congruency;
level of control by child or practitioner and control of events and routines.
S Self-Monitoring: Moving children from dependence on external cues and supports to
a self-directed and internally organized ability to modify their own behavior and manage
challenges
I Interactions: Interpersonal interaction style, including responses to supportive,
nurturing styles vs. more challenging, and demands or expectations for engagement (i.e.,
passive awareness to active collaboration)
60.
GOAL: TO IMPROVEHANDWRITING SKILLS BY SUPPORTING FINE MOTOR CONTROL,
POSTURAL STABILITY, AND ATTENTION THROUGH SENSORY INTEGRATION.
S – Sensation:
Provide proprioceptive and tactile input before writing:
Wall pushes
Finger warm-up with theraputty
Tracing shapes in sand or shaving cream to wake up tactile and visual systems
These help regulate the nervous system and prepare hands for fine motor tasks like pencil grasp and
pressure control.
61.
T –Task:
Set up a multi-sensory handwriting station:
First, trace large letters on a vertical surface (easel or chalkboard – builds shoulder stability)
Then, write letters in a tray of rice (tactile feedback)
Finally, move to paper-and-pencil writing tasks, focusing on letter formation and spacing
• Task is leveled from gross to fine motor and builds up to functional handwriting.
E – Environment:
Provide a structured and distraction-free workspace:
Foot support and correct chair/table height
Pencil grips or adaptive tools as needed
Visual cues for letter formation (e.g., highlighted lines, letter boxes)
62.
P –Predictability:
Use a consistent routine (e.g., "First warm-up, then writing game, then journal"). Visual schedule and checklists help the child anticipate
steps and transitions.
S – Self-Monitoring:
Use a self-check tool like a smiley face rating scale or a “Handwriting Hero” chart where the child evaluates:
“Did I sit up straight?” , “Did I hold my pencil correctly?” , “Did I keep my letters in the lines?”
This encourages awareness and builds self-correction over time.
I – Interactions:
The therapist offers guided support during early stages, modeling good posture and grip, then fades assistance to encourage
independence. Occasional “copy me” games or peer writing races can make it fun and social.
63.
A SECRET
ByLucy J. Miller, PhD, OTR/L, FAOTA
A SECRET is predicated on the notion that families and children can manipulate any of
seven elements to solve problems wherever and whenever they arise—at home, in
school, or in the larger community. The acronym provides an easy way to remember
and use problem-solving fundamentals in everyday life. The seven elements of the
acronym are as follows:
A Attention S Sensation E Emotion regulation C Culture
R Relationships E Environment T Tasks
64.
The firstthree elements—attention, sensation, and emotion regulation—are internal
characteristics that influence a child (i.e., internal dimensions). The last four elements—
culture, relationships, environment, and tasks—are the contextual elements that influence
a child from the outside (i.e., external dimensions).
A SECRET is an example of a reasoning tool that extends SI theory to families and
children for use in everyday activities and routines.
65.
A : Isthere a way I can draw my child’ s (or my) attention away from this problem?
S : Is there a sensation that is alarming my child (or me) right now? If so, what is it,
and can it be modified? Can I use another sensation to override the alarming one?
E: What emotion is my child (or am I) experiencing, and what techniques do I know to
support emotion regulation for the child (or myself) that work when the child feels (or I
feel) this way?
C: What part of the culture (context) can be changed to avoid situations such as this in
the future? For example, upsets in the grocery store: Could I do this activity without my
child? Could we do something to change the activity or context to make it easier or
more pleasant for my child (or for me) (e.g., couple the activity with a task such as
matching coupons to items selected at the store)?
66.
R :Is there something in a relationship with me or someone else right now
that’ s causing my child (or me) to act this way? What can I do about it? Or
how can I use the power of my relationship to lessen the situation?
E : What in the environment is setting off my child (or me)? How can I
modify it? Or is there something in the environment I can use to help my child
(or myself)?
T : What is troubling my child (or me) about the task at hand? How can the
task be modified so that it is not so problematic for my child (or me)? Is there
a task that I can use to provide a calming influence? For example, the problem
area is that the child is unable to maintain regulation during a worship service.
Can I discover what tasks will keep the child engaged (e.g., a color-by number
or dot-to-dot activity)?
67.
1. Gathering assessmentdata
2. Goal setting : Identify presenting problem,
underlying problem, and
desired functional outcome
3. Ongoing review process with family : to identify specific areas for intervention,
communicate their role with other members of the team, and monitor the effectiveness of
the chosen intervention strategies
SETTING GOALS FOR INTERVENTION
68.
The physicalenvironment needs to have adequate space to allow for the flow of
vigorous activity.
The arrangement of the equipment and materials needs to be flexible enough to allow
for rapid changes in configuration during an intervention session.
Safety must be maintained at all times in the therapy environment.
THE PHYSICAL ENVIRONMENT OF
INTERVENTION
69.
The useof mats, cushions, and pillows that are used to pad the floor underneath
all suspended equipment.
Equipment should be adjustable to the size of the child. All equipment must be
routinely checked for safety.
Therapists should take great care in self-monitoring their own safe use of
equipment.
The therapist may adjust the height, distance, or location of equipment to
prevent the child from bumping into hard surfaces, a wall, or a person.
The therapist may move mats or pillows to where the child might fall.
70.
1. Bouncing equipment
2.Rubber strips or ropes for pulling
3. Therapy balls
4. Platform swing
5. Platform glider
6. Frog swing
7. Scooter board and ramp
8. Flexion disc
9. Bolster swing
10. Tire swing
11. Weighted objects such as balls or bean
bags in various sizes
12. Inner tubes
13. Spandex fabric
14. Crash pillows
15. Ball pit
16. Vibrating toys or massagers
17. Various tactile materials
18. Visual targets
19. Climbing equipment
20. Barrel
21. Props to support engagement in play
(dress up clothes, sports equipment dolls,
and puppets)
22. Materials for practicing daily living skills
(school tools, clothing, hygiene, and other
home-related objects)
72.
While consideringwhich sensory systems to focus on (i.e., tactile,
vestibular, proprioceptive), a therapist also must consider the intensity
of the sensation.
Qualities of sensation influence intensity: Strength
Rhythmicity
Duration
Frequency
Speed
Qualities Affecting the Intensity of Sensation
73.
Strength isthe force with which sensation is administered. Touch, for
example, can be soft or firm.
Rhythmicity is the regularity of repetition of the sensation. For example, a
swing yields rhythmic input when a child propels it smoothly back and forth
or rhythmic input.
Duration is the length of time a sensation is present
Frequency is how often a sensation occurs
Speed refers to the rate of stimulus occurrence. For example, touch can be
slow as in stroking one’s arm or fast as in a tickling. Similarly, movement of
a body’s muscles and joints can also occur at various speeds.
74.
THERAPEUTIC INTERVENTIONS RELATEDTO
MODULATION
The therapist provides the child with various sensory opportunities,
with the intent of providing at least two of the following three types of
sensation: tactile, vestibular, and proprioceptive.
These sensations are provided beyond the normal presentation of
sensation that a child experiences in daily life and are graded to a
greater or lesser intensity depending on the needs of the child.
75.
When treatinga child with tactile over-responsivity or
defensiveness, Textures may be introduced in a graded manner,
starting with less bothersome textures, usually in combination with
deep pressure, proprioceptive, and/or vestibular activities.
Vestibular stimulation is often needed before, during, and after tactile
play to help the child stay calm and organized.
76.
Children whodemonstrated high arousal can be treated with the use of heavy
work activities, such as movement against weight or resistance.
The therapist can use deep touch pressure, with activities such as hugging, a
massage, or squeezing between objects, which may be calming for some
children.
Decreasing light touch can also help decrease arousal. Reducing other sensory
stimuli such as visual clutter, bright lights, and simultaneous auditory stimuli
The use of light or intermittent touch tends to be alerting. This can be provided
through activities that utilize objects which provide light, intermittent touch such
as playing dress up with a feather scarf, or by playing in a large ball pit that is
filled with textured objects rather than small hard balls.
78.
For childrenwith low arousal in the vestibular system, the therapist
would use fast, irregular (stop/start),and rotational movement, as
these tend to be alerting.
For children with high arousal in the vestibular system, the
therapist would use slow, linear, and rhythmical movement as such
movements tend to be calming.
79.
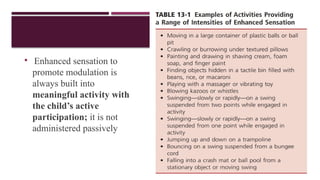
Enhanced sensationto
promote modulation is
always built into
meaningful activity with
the child’s active
participation; it is not
administered passively
83.
Heavy workactivates the proprioceptive system by increasing the load
on the muscles, requiring greater contraction of more muscle fibers and
producing greater tension on the tendons.
Heavy work can be incorporated through activities (such as a prone
position in a net swing), weight bearing (such as climbing up an
inclined ramp in quadruped), or increasing the weight that the child
must negotiate during daily activities (such as using a backpack filled
with books in it to walk from the classroom to the lunch room).
85.
To improvesomatodyspraxia,it is helpful to use proprioceptive
activities to increase unconscious and conscious awareness of
body position and body movement.
This may be accomplished through practice with motor activities,
use of a mirror while performing activities, and having the
therapist and child talk through an activity to motor plan various
novel activities.
86.
Tactile stimulationthat forms the basis for somatodyspraxia includes
providing the child with opportunities to encountering rich and varied
stimuli to the skin, such as textured materials, while the child is
performing motor actions. This helps to increase tactile feedback and
awareness of one’s body parts.
Specific examples include stepping on, crawling over, hanging on,
or moving through textured items such as fabrics, sheets, shaving
cream, and so on.
Rubbing textured items on the body before or during motor activities
also helps to increase tactile awareness of one’s body.
87.
Modulation ofsensory stimuli is an important component of
obtaining and maintaining optimal arousal level.
Optimal arousal enables the child to participate in the activities
with appropriate alertness, attention, comfort, and activity
level.
An optimal arousal level is necessary for the child to access
environmental and sensory opportunities.
88.
THERAPEUTIC INTERVENTIONS RELATEDTO SENSORY
DISCRIMINATION
Sensory discrimination is the natural next step after sensory modulation.
Many of the techniques used for intervention in sensory modulation also apply to sensory
discrimination.
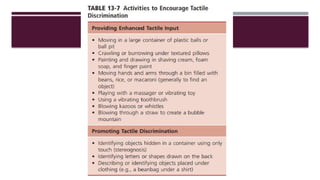
To help a child develop appropriate tactile discrimination, the child may discriminate size,
shape, texture, location, and quality of a variety of tactile stimuli to various areas of the
body with and without vision.
For example, the child explores, feels, and identifies key aspects of objects without
vision such as finding toys hidden in rice, guessing objects without seeing them, and
finding a particular object in a container with other objects.
90.
VESTIBULAR-PROPRIOCEPTIVE DISCRIMINATION
Thevestibular and proprioceptive systems are responsible for
understanding body position in and movement through space,
maintaining posture, and maintaining a stable visual field.
Poor discrimination of vestibular and proprioceptive sensation is
manifest in several ways but most commonly as difficulty with
postural control: stabilizing or adjusting the body to meet the
demands of a task or a changing environment.
91.
Developing Postural Control
Tonic postural control depends on interplay between flexor and extensor muscles;
it begins to develop in infancy, first in neck extensor muscles and proceeding to
trunk extensors.
Intervention to improve tonic postural control includes enhanced vestibular and
proprioceptive sensations and challenges to posture..
Activities incorporate linear vestibular input and resistance to movement.
Linear movement can occur in any plane: anterior or posterior (e.g., swinging to
and fro); horizontal (e.g., swinging side-to-side); or vertical (e.g., bouncing).
94.
THERAPEUTIC INTERVENTIONS RELATEDTO
BILATERAL INTEGRATION AND SEQUENCING
Children who are experiencing deficits in bilateral integration and
sequencing require the therapist infuse vestibular input into
activities involving increasing complexity of bilateral
coordination and the timing of body movements.
Common activities include targeting objects while in motion or
coordinating one’s body movements in time to achieve specified
outcomes.
Many skills that require bilateral coordination also involve
projected action sequences (e.g., catching a ball with two hands).
95.
To developpostural, visual motor, visual perceptual skills, and bilateral
integration, the therapist will provide various opportunities that are challenging
to the child.
This includes activities that will promote postural responses while in motion,
the use of visual feedback while moving, and the use of two hands together.
These activities are devised to be fun for the child so that the child will
concentrate on the activity and responding, rather than thinking about using both
hand together or maintaining his or her balance while in motion.
96.
THERAPEUTIC INTERVENTIONS RELATEDTO PROMOTING
PRAXIS
To encourage the ability to create ideas for planning and executing new and
unfamiliar motor activities within the context of play, the therapist supports
and guides the child’s self-organization of behaviour during play activities.
This is accomplished by assuring that child-directed activities are a good
match for the child’s developing skills and abilities (the just right challenge)
and covertly adjusts the environmental demands to ensure that the activity
is successful.
97.
The therapistpresents or supports activities in which the child can be
successful in response to sensory, motor, cognitive, or social challenge.
The therapist allows the child to experience success in doing part or all of an
activity.
This promotes the development of self-esteem and self-confidence.
Ultimately, involvement in such activities will facilitate self-regulation to
provide positive and appropriate sensory and motor feedback utilized to
develop body awareness and praxis.
98.
SENSORY INTEGRATION THERAPYFOR CHILDREN WITH AUTISM SPECTRUM DISORDER
ASD is one of the most frequently occurring neurodevelopmental disorders in
children, with current prevalence estimates suggesting that 1 in 68 children have an
ASD diagnosis .
The recent change in diagnostic criteria for the DSM-5 ( APA, 2013a ) for the
first time acknowledges and recognizes the frequency with which sensory
processing differences and challenges are reported in people with ASD
Similarly, motor and praxis symptoms are frequently reported and have been
studied.
99.
Sensory modulationchallenges, sensory discrimination dysfunction, and
sensory-based motor problems including dyspraxia and postural disorders
are commonly seen in children with ASD.
Occupational therapists focus on occupational performance in daily life
activities. In children with ASD, differences in sensory responsivity have
been linked to reduced participation in a variety of occupational areas, such as
social participation, play, and performance of self-care skills, such as
bathing, dressing, and feeding.
Assessment of sensory integrative function in children with ASD can be
accomplished using the SIPT, tools addressing sensory modulation, and
clinical observations.
100.
One commonapproach to addressing sensory symptoms in children with autism is
using ASI.
Ayres (1972 ) proposed that information from the tactile, vestibular, and
proprioceptive systems were important substrates for adaptive responses and that
difficulty processing and integrating sensations from the body and environment
contribute to disrupted or disorganized motor skills and adaptive behaviors.
Occupational therapy using SI focuses on improving sensory symptoms that impact
behavior and addresses underlying sensory and motor factors that may be affecting
occupational performance.
Emerging evidence suggests that using a sensory integrative approach and
abiding by tenets as proposed by Ayres ( 1979) and explicated by Parham and
colleagues ( 2011) may positively influence functional outcomes of children with
101.
SENSORY INTEGRATION THERAPYFOR CHILDREN
WITH WITH ATTENTION DEFICIT-HYPERACTIVITY
DISORDER
ADHD is placed within the section describing neurodevelopmental disorders in
the Diagnostic and Statistical Manual for Mental Disorders, ( DSM-5; APA,
2013b) , and it is characterized by persistent and maladaptive symptoms of
inattention, hyperactivity, and impulsivity.
Children with ADHD have an increased risk of sensory modulation difficulties
(sensory over-responsivity [SOR] or sensory under-responsivity [SUR]) as well as
deficits in visual perception .
102.
Studies haveshown that ADHD is associated with adverse reactions to tactile stimuli
and motor planning problems.
Mulligan also demonstrated postural control and balance deficits, sensory-based
dyspraxia, and visual-motor integration difficulties in this group of children
( Mulligan, 1996 ).
More recently, Pfeiffer, Daly, Nicholls, and Gullo ( 2 015) found that children with
ADHD were much more likely to exhibit challenges in all areas of sensory processing
than those of neuro-typical children and to display problems with higher level
functions believed to be dependent in part on efficient sensory processing,
including social participation and motor planning.
103.
Comprehensive evaluationsof children with ADHD using an SI approach include
administration of the Sensory Integration and Praxis Test (SIPT; Ayres, 2 005) , a
measure of sensory modulation such as the SP ( Dunn, 2014 ), clinical observations, as
well as gathering information through interviews and naturalistic observations when
possible
SI is a useful treatment approach for children with ADHD if specific patterns of SI
dysfunction have been identified.
During intervention sessions, it is important to emphasize sensory activities that aim to
regulate the child’s level of arousal throughout the session as well as those aimed at
addressing specific problems, such as dyspraxia or visual motor integration deficits.
104.
Treatment spacesmay be better able to meet the child’s needs if they are free from
clutter to minimize distractions and the potential for the child to become
overstimulated.
Allowing the child to choose those activities that he or she enjoys is vital, as children
with ADHD may only be able to attend to tasks well when they are invested in or
interested in whatever they are doing
105.
REFERENCES
1. Sensory IntegrationTheory and Practice, 2nd
and 3rd
edition , Anita Bundy , Shelly
Mulligan
2. Frames of References for Paediatric Occupational Therapy, edition, Paula Kramer.
3. Case Smith’s Occupational Therapy for Children and Adolescents, 8th
edition.






![SENSORY INTEGRATION THERAPY FOR CHILDREN
WITH WITH ATTENTION DEFICIT-HYPERACTIVITY
DISORDER
ADHD is placed within the section describing neurodevelopmental disorders in
the Diagnostic and Statistical Manual for Mental Disorders, ( DSM-5; APA,
2013b) , and it is characterized by persistent and maladaptive symptoms of
inattention, hyperactivity, and impulsivity.
Children with ADHD have an increased risk of sensory modulation difficulties
(sensory over-responsivity [SOR] or sensory under-responsivity [SUR]) as well as
deficits in visual perception .](https://image.slidesharecdn.com/sensoryintegrationforeasa-250806162945-6715668a/85/THE-SENSORY-INTEGRATION-APPROACH-OCCUPATIONAL-THERAPY-101-320.jpg)