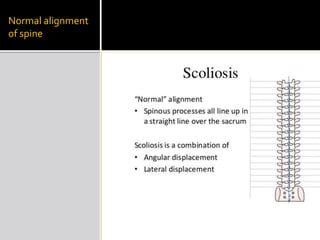
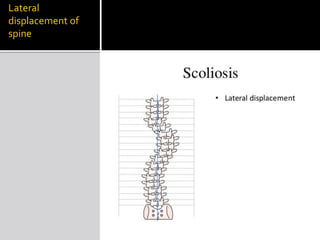
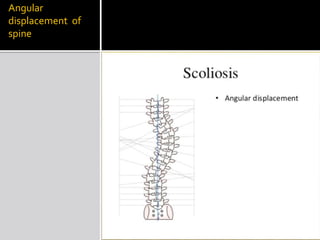
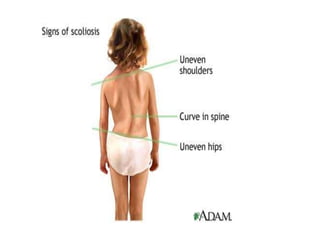
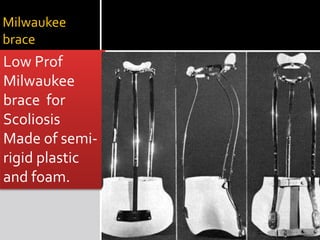
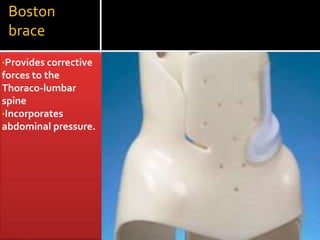
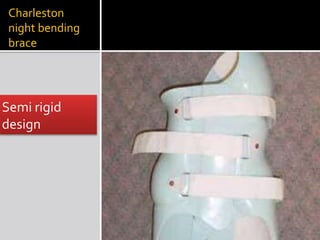
Scoliosis is a lateral curvature of the spine. It can be classified as mild (less than 20 degrees), moderate (20-40 degrees), or severe (over 40 degrees). Treatment depends on the severity and may include bracing or surgery. Common bracing options are the Milwaukee brace, TLSO brace, and Charleston night brace. The goals of bracing are to prevent curve progression in growing children and avoid the need for surgery.