Downloaded 23 times
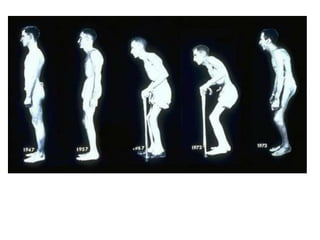




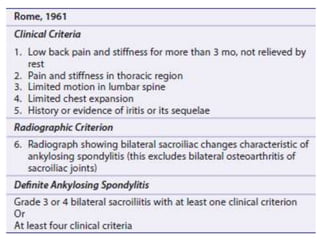
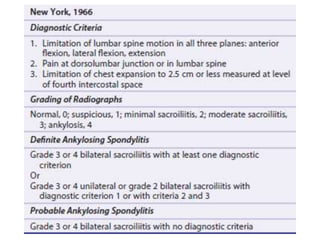
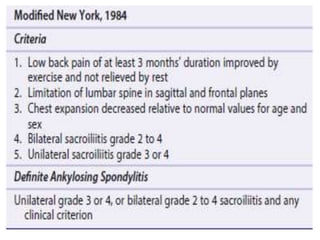
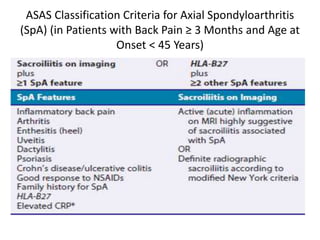



This document provides information on Ankylosing Spondylitis (AS), including: - It is an inflammatory arthritis affecting the spine and sacroiliac joints, causing stiffness and fusion of the joints. HLA-B27 gene and TNF play a role in its pathogenesis. - Signs and symptoms include back pain, limited spinal mobility, chest expansion and peripheral joint involvement. Imaging shows bone erosion and formation in affected areas. - Treatment involves exercise, NSAIDs, and biologics targeting TNF. Surgery may be needed in advanced cases to correct deformities.













































































