Downloaded 343 times
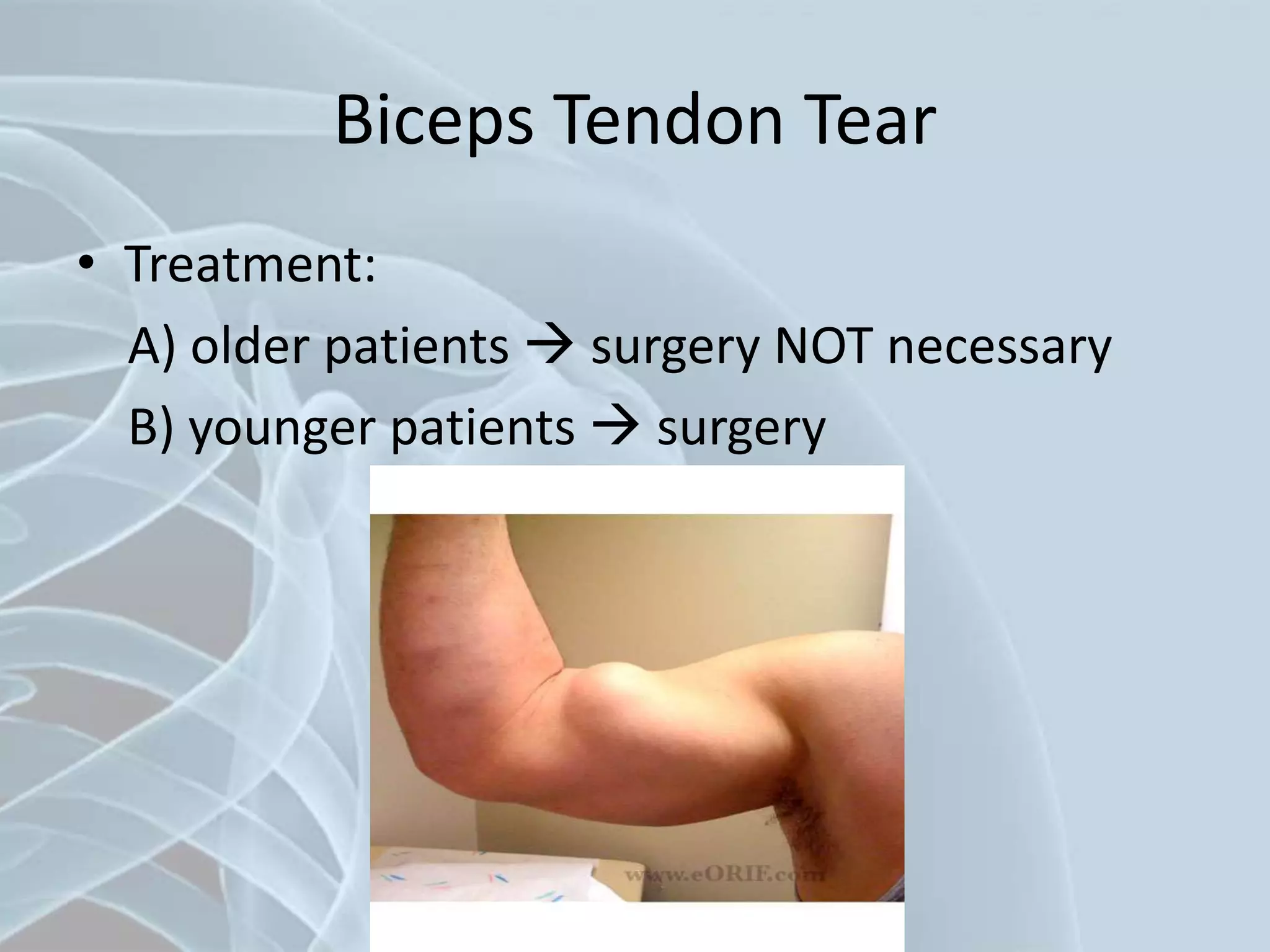
















The document provides a comprehensive overview of various shoulder disorders, including anatomy, symptoms, diagnostic procedures, and treatment options. Key conditions discussed include biceps tendon tears, frozen shoulder, rotator cuff tears, and impingement syndrome, each characterized by specific clinical presentations and recommended management strategies. Diagnostic techniques range from physical examinations and radiography to MRI and arthroscopy, with treatment options varying from conservative methods to surgical interventions.

































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)















