
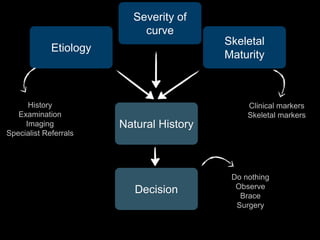

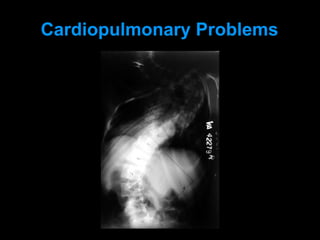



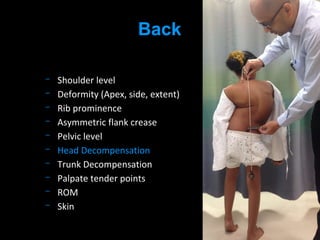
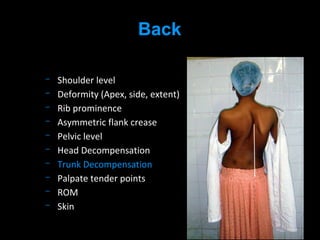
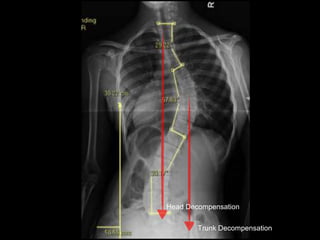
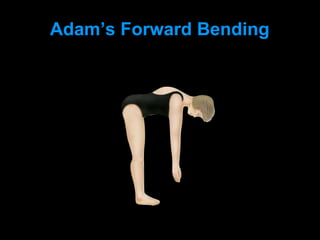

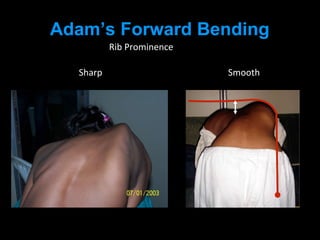
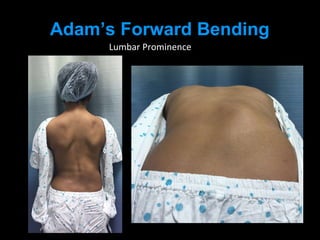
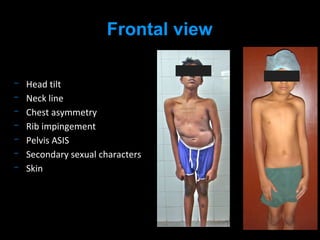
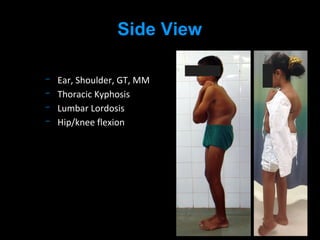





1) A thorough workup for scoliosis includes obtaining a detailed history, performing a physical examination, and ordering imaging studies. The history should include questions about deformity, pain, neurological symptoms, cardiopulmonary issues, and family history. 2) The physical examination evaluates posture, spinal alignment, and flexibility from multiple angles. It also evaluates the shoulders, ribs, pelvis, and for any neurological deficits. 3) Imaging studies like x-rays can further characterize the curve severity, skeletal maturity, and help determine a treatment plan. Together the history, exam, and imaging allow for an accurate diagnosis and clinical decision making.































































































