A randomized clinical trial compared the effects of a low-fat vegan diet versus a diet following American Diabetes Association (ADA) guidelines on glycemic control and cardiovascular risk factors in individuals with type 2 diabetes. 99 participants were randomly assigned to either a low-fat vegan diet or an ADA diet for 22 weeks. The vegan diet resulted in greater reductions in A1C, body weight, LDL cholesterol, and urinary albumin compared to the ADA diet. Both diets improved glycemic and lipid control, but improvements were greater with the low-fat vegan diet.

![Low-fat vegan diet and type 2 diabetes
favor low– glycemic index foods, such as 24-h recalls or incidentally at any point, ence was measured at the maximal pro-
beans and green vegetables. Portion sizes, as saturated fat Յ5% and total fat Յ25% trusion of the buttocks.
energy intake, and carbohydrate intake of energy, and as average daily cholesterol Blood pressure was measured after
were unrestricted. intake Յ50 mg on 3-day dietary records participants had rested in a seated posi-
The ADA diet (15–20% protein, Ͻ7% at 22 weeks. Adherence for the ADA tion for 5 min using a digital monitor
saturated fat, 60 –70% carbohydrate and group was defined as average daily energy (Omron HEM-711) and a standard cuff
monounsaturated fats, and cholesterol intake on the 22-week 3-day dietary maintained at the level of the heart. Three
Յ200 mg/day) was individualized, based records being no more than 200 kcal in measurements were taken at 2-min inter-
on body weight and plasma lipid concen- excess of the intake prescribed by the reg- vals; the first measurement was disre-
trations (6). ADA group participants with istered dietitian and saturated fat Յ10% garded, and a mean was calculated for the
a BMI Ͼ25 kg/m2 (all but three ADA of energy. Individuals who attended remaining two values.
group participants) were prescribed en- fewer than 10 of the 22 weekly sessions
ergy intake deficits of 500 –1,000 kcal. were also considered nonadherent on ei- Statistical analyses
No meals were provided. To meet the ther diet. To have an 80% chance of detecting a
vitamin B12 needs of the vegan group Participants were asked to continue 1.5–percentage point between-group
while maintaining the same intervention their preexisting medication regimens, A1C difference as significant (at the two-
in the ADA group, all participants were except when fasting plasma glucose deter- sided 5% level), with an assumed SD of
provided a vitamin B12 supplement (100 minations fell below 4.4 mmol/l or hypo- 1.9% and a loss to follow-up of 26%, 34
g) to be taken every other day. For both glycemic symptoms were accompanied participants were required per group. An
groups, alcoholic beverages were limited by a capillary glucose reading Ͻ3.6 interim analysis indicated group differ-
to one per day for women and two per day mmol/l. In such cases, medications were ences of 0.8% with an SD of 1.3%; there-
for men. Participants were asked not to reduced for participant safety by a study fore, a revised power analysis was
alter their exercise habits during the inter- endocrinologist, who remained blind to conducted. To have an 80% chance of de-
vention period. group assignment, following an estab- tecting a 0.8% difference as significant
Each participant met for 1 h with a lished protocol. with an SD of 1.3% and loss to follow-up
registered dietitian experienced in the use Laboratory measurements were made of 33%, an additional 15 participants
of the assigned diet to establish an appro- after a 12-h fast by technicians blind to were required per group.
priate diet plan. Thereafter, participants group assignment. A1C (the primary end Between-subject t tests were calcu-
attended weekly 1-h meetings of their as- point) was assayed at 0, 11, and 22 weeks, lated for each measure to determine
signed groups for nutrition and cooking as described above. All other measures whether the changes associated with the
instruction conducted by a physician and were assessed at baseline and 22 weeks, intervention diet were greater than those
a registered dietitian and/or a cooking in- except as noted. Plasma glucose was mea- associated with the control diet. Within
structor. Sessions for the two groups were sured by the glucose oxidase method us- each diet group, paired comparison t tests
similar in duration and content, except ing an Abbott Spectrum analyzer (Abbott were calculated to test whether the
with regard to dietary details. Group lead- Park, IL) (8). Plasma cholesterol and tri- change from baseline to 22 weeks was sig-
ers were instructed to make no comment glyceride concentrations were measured nificantly different from zero. The pri-
favoring either diet over the other. by enzymatic methods using an Abbott mary analysis of the main end point was
At weeks 4, 8, 13, and 20, a registered Spectrum analyzer (9,10). HDL choles- intention to treat and included all partic-
dietitian made unannounced telephone terol was measured after double precipi- ipants. Because medication changes influ-
calls to each participant to administer a tation with dextran and MgCl2 (11). LDL ence the dependent measures,
24-h diet recall. These recalls were not cholesterol was estimated using the exploratory analyses were performed for
statistically analyzed, but allowed the in- Friedewald equation (12). In individuals the subgroup whose medications re-
vestigators to check for poor adherence whose plasma triglyceride concentrations mained constant. An ␣ of 0.05 was used
and provide additional dietary counseling exceeded 400 mg/dl, LDL cholesterol was for all statistical tests, with no adjustment
as needed. measured directly by precipitation and for multiple comparisons.
In addition, a 3-day dietary record magnetic separation (LipiDirect; Poly- Regression analyses assessed whether
was completed by each participant at medco, Cortlandt Manor, NY). Non-HDL the diet group effects on A1C and body
weeks 0, 11, and 22, on 2 weekdays and 1 cholesterol concentration was calculated weight were significant, while controlling
weekend day, using a food scale, after par- as the difference between total and HDL for baseline values, and whether the diet
ticipants had completed a 3-day practice cholesterol. Urinary albumin was mea- group effect on A1C was significant, while
record. Using the Nutrition Data System sured on 24-h samples using an anionic controlling for baseline A1C and changes
for Research software version 5.0 (Food dye– binding assay (13). in body weight. Pearson correlations were
and Nutrient Database 35 [released May Physical activity was assessed over a calculated for the relationship between
2004]; Nutrition Coordinating Center, 3-day period by pedometer (Omron HJ- A1C change and weight change.
University of Minnesota, Minneapolis, 112) and with the Bouchard 3-Day Phys- An interim analysis was performed af-
MN) (7), a registered dietitian certified by ical Activity Record (14). Body weight ter week 11 to assess whether benefits
Note the use of
the Nutrition Coordinating Center ana- was determined at 0, 11, and 22 weeks, or adverse outcomes were statistically
lyzed all 3-day dietary records and diet structured headings
before breakfast while participants wore unusual.
recalls. For purposes of statistical analy- (research design a digital scale accu-
hospital gowns, using
sis, dietary adherence for the vegan group and methods,Waist circumference was
rate to 0.1 kg. RESULTS — Of 1,049 individuals
was defined as the absence of meat, poul- measured with a tape measure placed 2.5 screened by telephone, 99 met participa-
try, fish, dairy, or egg intake reported on results, conclusions, Hip circumfer-
cm above the umbilicus. tion criteria and were randomly assigned
etc.)
1778 DIABETES CARE, VOLUME 29, NUMBER 8, AUGUST 2006](https://image.slidesharecdn.com/vegan2annotated-120621110137-phpapp02/85/Scholarly-Article-2-320.jpg)
![Barnard and Associates
Table 1—Baseline demographic and clinical variables g/day, P Ͻ 0.0001; ADA 23 Ϯ 12 to 14 Ϯ
6 g/day, P Ͻ 0.0001 [between-group P Ͻ
Vegan group ADA group P value 0.001]) and cholesterol (vegan 291 Ϯ
223 to 24 Ϯ 57 mg/day, P Ͻ 0.0001; ADA
n 49 50 317 Ϯ 200 to 189 Ϯ 89 mg/day, P Ͻ
Age (years) 56.7 (35–82) 54.6 (27–80) 0.29 0.0001 [between-group P ϭ 0.002]). Fi-
Sex 0.26 ber increased only among vegans (18.8 Ϯ
Male 22 (45) 17 (34) 6.4 to 36.3 Tables g/day, P Ͻ 0.0001;
Ϯ 13.3 of results
Female 27 (55) 33 (66) ADA 19.5 Ϯ 6.9 to 19.0 Ϯ 7.9 g/day, P ϭ
Race, ethnicity 0.71* 0.73 [between-group P Ͻ in
are typical 0.001]).
Black, non-Hispanic 22 (45) 22 (44) scholarly articles.
Pedometer readings and self-reported
White, non-Hispanic 21 (43) 22 (44) energy expenditure revealed no signifi-
White, Hispanic 4 (8) 2 (4) cant between-group differences. Group-
Asian, non-Hispanic 2 (4) 4 (8) specific dietary adherence criteria were
Marital status 0.08 met by 67% (33 of 49) of vegan group
Not married 20 (41) 26 (52) participants and 44% (22 of 50) of ADA
Married 29 (59) 24 (48) group participants. During the interven-
Education 0.69 tion period, 43% (21 of 49) of vegan
High school, partial or graduate 6 (12) 3 (6) group participants and 26% (13 of 50) of
College, partial or graduate 26 (53) 25 (50) ADA group participants reduced their di-
Graduate degree 17 (35) 22 (44) abetes medications, mainly as necessi-
Occupation 0.04 tated by hypoglycemia, while 8% (4 of
Service occupation 3 (6) 7 (14) 49) of vegans and 8% (4 of 50) of ADA
Technical, sales, administrative 16 (33) 18 (36) participants increased medications with-
Professional or managerial 15 (31) 21 (42) out investigators’ authorization.
Retired 15 (31) 4 (8) A1C fell 0.96 percentage points (P Ͻ
On insulin 11 (22) 5 (10) 0.09 0.0001) in the vegan group and 0.56 per-
On metformin 34 (69) 39 (78) 0.33 centage points (P ϭ 0.0009) in the ADA
On sulfonylurea 25 (51) 29 (58) 0.49 group (between-group P ϭ 0.089; base-
On thiazolidinedione 16 (33) 15 (30) 0.78 line-adjusted P ϭ 0.091; Table 2 and Fig.
On other diabetes medications 1 (2) 2 (4) 0.57 1). Among participants whose diabetes
On blood pressure medications 31 (63) 38 (76) 0.17 medications remained unchanged
On lipid-lowering medications 27 (55) 27 (54) 0.88 throughout (n ϭ 24 vegan and n ϭ 33
History of eye involvement 9 (18) 10 (20) 0.82 ADA), A1C fell 1.23 points in the vegan
History of renal involvement 6 (12) 4 (8) 0.48 group and 0.38 points in the ADA group
History of neuropathy 18 (37) 24 (48) 0.25 (P ϭ 0.01; baseline-adjusted P ϭ 0.007).
Mean BMI (kg/m2) 33.9 35.9 0.18 Subanalyses were conducted to assess the
Ͻ25 kg/m2 5 (10) 2 (4) effects of dietary adherence. For those
25–29.9 kg/m2 14 (29) 5 (10) who met adherence criteria (n ϭ 33 vegan
Ն30 kg/m2 30 (61) 43 (86) and n ϭ 22 ADA), the A1C changes were
Data are mean (range) or n (%) unless otherwise indicated. P values refer to t test for continuous variables and Ϫ1.20% for the vegan group and
2 for categorical variables. *P value calculated for race distribution; for ethnicity (Hispanic vs. non-His- Ϫ0.88% for the ADA group (P ϭ 0.31).
panic), P ϭ 0.39.
For those who were both adherent and
medication stable (n ϭ 17 vegan and n ϭ
to the vegan (n ϭ 49) or ADA (n ϭ 50) duced energy intake (vegan 1,759 Ϯ 468 12 ADA), A1C changes were Ϫ1.48% for
groups. The reasons for exclusion were to 1,425 Ϯ 427 kcal/day, P Ͻ 0.0001; the vegan group and Ϫ0.81% for the ADA
A1C values outside the required range ADA 1,846 Ϯ 597 to 1,391 Ϯ 382 kcal/ group (P ϭ 0.15).
(n ϭ 201), failure to meet other participa- day, P Ͻ 0.0001 [between-group P ϭ To test whether the effect of diet on
tion criteria (n ϭ 279), inability to attend 0.22]) and protein intake (vegan 77 Ϯ 27 A1C was mediated by body weight
scheduled meetings (n ϭ 187), failure to to 51 Ϯ 16 g/day, P Ͻ 0.0001; ADA 85 Ϯ changes, a regression model was con-
keep interview appointment (n ϭ 153), 27 to 73 Ϯ 23 g/day, P ϭ 0.002 [between structed, including baseline A1C, weight
reluctance to change diet (n ϭ 72), and group P ϭ 0.01]). Carbohydrate intake change, and diet group as predictors of
other or unspecified (n ϭ 58). The partic- increased in the vegan group from 205 Ϯ A1C change, among those whose hypo-
ipants’ demographic and clinical charac- 69 to 251 Ϯ 70 g/day (P Ͻ 0.0001) but glycemic medications remained constant.
teristics (Table 1) were similar to those of fell in the ADA group from 213 Ϯ 70 to In this model, the effect of diet group was
individuals with type 2 diabetes in the 165 Ϯ 51 g/day (P Ͻ 0.0001 [between- no longer significant (P ϭ 0.23). Control-
Washington, DC, area. All participants group P Ͻ 0.001]). ling for diet group and for baseline A1C
completed laboratory assessments at 22 Fat intake fell in both groups (vegan scores, weight change was significantly
weeks. 72 Ϯ 28 to 30 Ϯ 19 g/day, P Ͻ 0.0001; associated with A1C change; each kilo-
Three vegan participants and eight ADA 73 Ϯ 35 to 52 Ϯ 21 g/day, P Ͻ gram of weight loss was associated with a
ADA participants failed to complete 22- 0.0001 [between-group P ϭ 0.002]), as 0.12% drop in A1C. For the subgroup
week dietary records. Both groups re- did saturated fat (vegan 23 Ϯ 10 to 6 Ϯ 4 that did not change diabetes medications,
DIABETES CARE, VOLUME 29, NUMBER 8, AUGUST 2006 1779](https://image.slidesharecdn.com/vegan2annotated-120621110137-phpapp02/85/Scholarly-Article-3-320.jpg)

![Barnard and Associates
Data are means Ϯ SD unless otherwise indicated. Listed P values are for comparisons of between-group (vegan vs. ADA) changes (baseline to 22 weeks).*P Ͻ 0.0001, †P Ͻ 0.001, ‡P Ͻ 0.01, and ʈP Ͻ 0.05 for
within-group changes. §Blood pressure was not determined on one vegan group participant due to equipment failure. ¶When triglycerides exceeded 400 mg/dl, LDL was calculated via direct-LDL; two ADA-group
the Pearson’s correlation of weight change
0.01
0.14
0.05
0.98
0.02
0.89
0.98
0.68
with A1C change was r ϭ 0.51, P Ͻ
0.0001 (within the vegan group [n ϭ 24],
r ϭ 0.39, P ϭ 0.05; within the ADA group
Ϫ14.5 (Ϫ25.8 to Ϫ3.2)
Ϫ11.9 (Ϫ22.2 to Ϫ1.7)
0.6 (Ϫ45.9 to 47.2)
Ϫ11.3 (Ϫ22.9 to 0.3) [n ϭ 33], r ϭ 0.49, P ϭ 0.004).
individuals were excluded due to lack of sufficient plasma samples. SI conversion: to convert HDL, LDL, and total cholesterol to mmol/l, multiply by 0.0259; for tryiglycerides, multiply by 0.0113.
Ϫ3.2 (Ϫ7.5 to 1.1)
Ϫ0.0 (Ϫ0.4 to 0.4)
0.4 (Ϫ4.8 to 5.6)
0.02 (Ϫ0.1 to 0.1)
Body weight fell 5.8 kg in the vegan
group (P Ͻ 0.0001) and 4.3 kg in the
ADA group (P Ͻ 0.0001) (between-group
P ϭ 0.082; baseline-adjusted P ϭ 0.066).
Among medication-stable participants,
vegan participants lost 6.5 kg compared
with 3.1 kg for ADA participants (P Ͻ
0.001; baseline-adjusted P ϭ 0.001).
Ϫ19.0 Ϯ 28.5*
Ϫ2.8 Ϯ 11.6
Ϫ16.3 Ϯ 30.1ʈ
Ϫ0.3 Ϯ 1.2
Ϫ10.7 Ϯ 23.3ʈ
Ϫ3.8 Ϯ 12.1
134.6 Ϯ 122.9 Ϫ22.8 Ϯ 134.3
Ϫ0.06 Ϯ 0.21
The reduction in urinary albumin was
significant in the vegan group (P ϭ 0.002)
but not in the ADA group (P ϭ 0.14). The
unadjusted between-group difference
was not significant. However, after adjust-
ment for baseline values, the effect of diet
175.9 Ϯ 36.2
46.4 Ϯ 12.2
129.4 Ϯ 35.9
4.0 Ϯ 1.3
104.6 Ϯ 33.7
21.7 Ϯ 9.0
2.05 Ϯ 0.24
was significant (P ϭ 0.013).
For the entire sample, there were no
between-group differences in lipid val-
ues. Among those whose lipid-controlling
medications remained constant (80% [39
of 49] of vegan group, 82% [41 of 50] of
25.5 Ϯ 13.2
157.4 Ϯ 143.0
2.11 Ϯ 0.25
194.9 Ϯ 40.9
49.2 Ϯ 15.5
145.7 Ϯ 42.9
4.4 Ϯ 1.8
115.3 Ϯ 40.4
ADA group), reductions in total choles-
terol were Ϫ0.866 mmol/l (Ϫ33.5 mg/dl,
Ϫ17.6%) for the vegan group and
Ϫ0.491 mmol/l (Ϫ19.0 mg/dl, Ϫ9.7%)
for the ADA group (P ϭ 0.0125). Changes
in LDL cholesterol were Ϫ0.58 mmol/l
Ϫ3.5 Ϯ 10.5ʈ
Ϫ22.2 Ϯ 58.5ʈ
Ϫ0.04 Ϯ 0.16
Ϫ33.5 Ϯ 21.5*
Ϫ6.0 Ϯ 6.8*
Ϫ27.6 Ϯ 21.1*
Ϫ0.3 Ϯ 0.6‡
Ϫ22.6 Ϯ 22.0*
(Ϫ22.6 mg/dl, Ϫ21.2%) for the vegan
group and Ϫ0.277 mmol/l (Ϫ10.7 mg/dl,
Ϫ9.3%) for the ADA group (P ϭ 0.023).
Changes in HDL cholesterol were Ϫ0.16
mmol/l (Ϫ6.0 mg/dl, Ϫ11.0%) for the
vegan group and Ϫ0.07 mmol/l (Ϫ2.8
23.1 Ϯ 10.9
118.2 Ϯ 57.3
2.02 Ϯ 0.22
156.9 Ϯ 25.1
48.6 Ϯ 18.4
108.3 Ϯ 25.6
3.6 Ϯ 1.2
84.6 Ϯ 22.5
mg/dl, Ϫ5.7%) for the ADA group (P ϭ
0.14). The total-to-HDL cholesterol ratio
fell for both groups, as did triglyceride
concentrations.
There were no treatment-related seri-
26.6 Ϯ 15.4
140.3 Ϯ 89.1
2.06 Ϯ 0.28
190.5 Ϯ 36.8
54.6 Ϯ 21.0
135.9 Ϯ 38.4
3.9 Ϯ 1.5
107.3 Ϯ 34.3
ous adverse events.
CONCLUSIONS — Both diets were
associated with significant clinical im-
provements, as indicated by reductions in
A1C, body weight, plasma lipid concen-
controlling medications (n ϭ 39 vegan,
VLDL cholesterol (n ϭ 38 n ϭ vegan, 38
LDL cholesterol (n ϭ 39 vegan, n ϭ 39
trations, and urinary albumin excretion.
Among medication-stable participants,
Participants with no changes to lipid-
changes in A1C, weight, BMI, waist cir-
n ϭ 41 ADA, except as noted)
Total cholesterol/HDL (mg/dl)
cumference, total cholesterol, and LDL
Non-HDL cholesterol (mg/dl)
cholesterol were significantly greater in
Total cholesterol (mg/dl)
HDL cholesterol (mg/dl)
the vegan group. The magnitude of A1C
Triglycerides (mg/dl)
reduction in medication-stable vegan
group participants, 1.23 percentage
Log triglycerides
ADA) (mg/dl)¶
points, compares favorably with that ob-
ADA) (mg/dl)
served in single-agent therapy with oral
diabetes drugs (15).
A low-fat plant-based diet influences
nutrient intake and body composition in
several ways that may, in turn, affect in-
DIABETES CARE, VOLUME 29, NUMBER 8, AUGUST 2006 1781](https://image.slidesharecdn.com/vegan2annotated-120621110137-phpapp02/85/Scholarly-Article-5-320.jpg)
![Low-fat vegan diet and type 2 diabetes
portions can, as a result, easily exceed rec-
ommended limits on saturated fat. In con-
trast, the vegan diet includes no animal
fat, so variations in food quantity are less
likely to result in substantial increases in
saturated fat intake. Because the vegan
diet is based on the elimination of certain
foods, it may be easier to understand than
regimens that limit quantities of certain
foods without proscribing any. The ac-
ceptability of low-fat vegan diets in clini-
cal studies is similar to that of seemingly
more moderate diets (27).
This study’s strengths include its
analysis of dependent measures without
regard to variations in dietary adherence
and applicability outside the research set-
ting. A study limitation was that both di-
ets made participants vulnerable to the
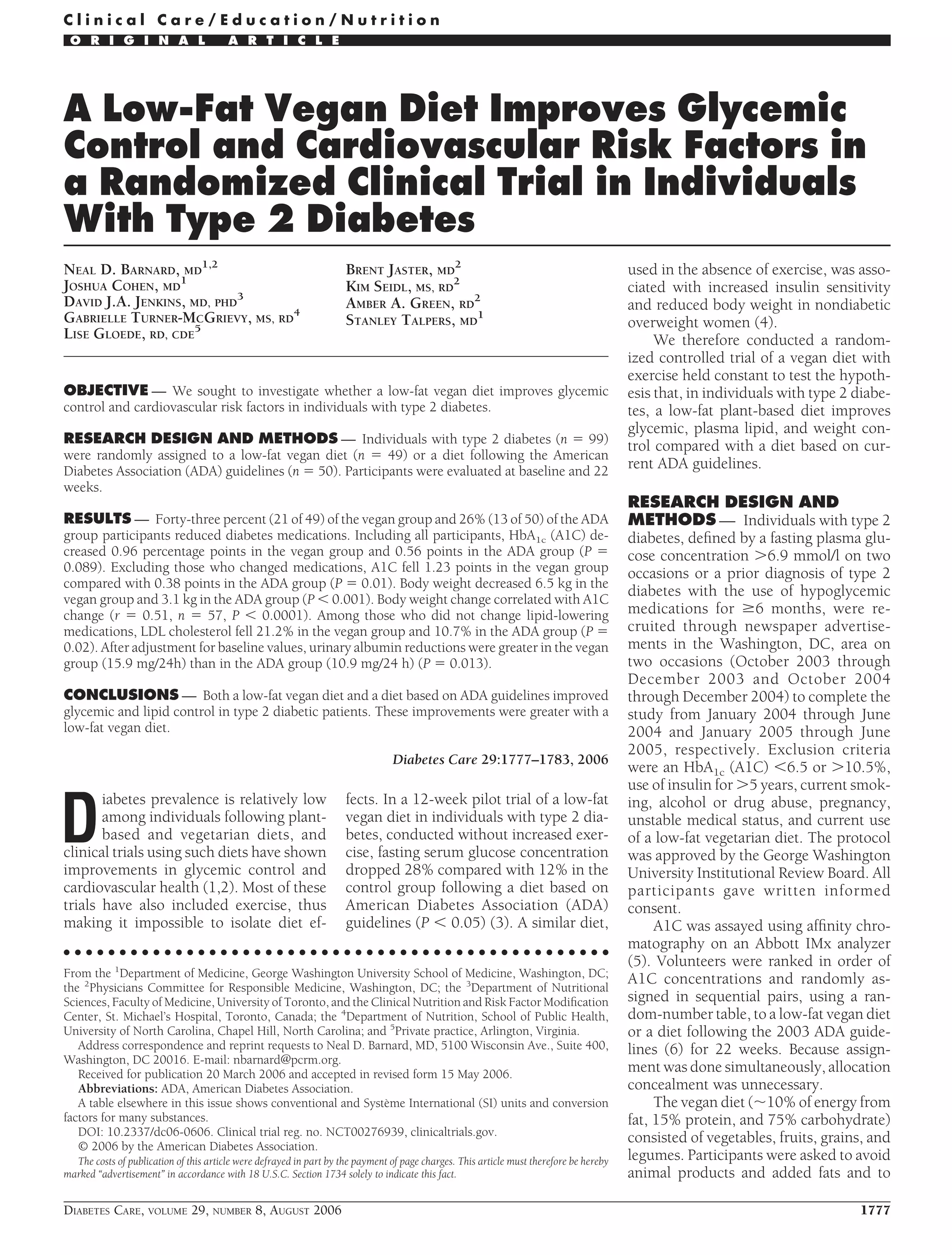
Figure 1—A1C at baseline and at 11 and 22 weeks. Open circles: all vegan group participants
hypoglycemic effect of their diabetes
(n ϭ 49); closed circles: medication-stable vegan group participants (n ϭ 24); open squares: all
ADA group participants (n ϭ 50); closed squares: medication-stable ADA group participants (n ϭ medications, resulting in medication re-
33). Error bars represent SE of the mean. P ϭ 0.09 for between-group comparison from baseline ductions that confound the interpretation
to 22 weeks for full sample; P ϭ 0.01 for medication-stable participants (vegan vs. ADA). of A1C changes and necessitating a sub-
group analysis of medication-stable par-
ticipants. Because these episodes
sulin sensitivity. First, because such diets fore diabetes manifests (20). This lipid occurred early in the trial, there was no
are low in fat and high in fiber, they typ- accumulation may be responsive to diet. opportunity to bring interim laboratory
ically cause associated reductions in di- High-fat diets appear to downregulate the values forward. Also, most study partici-
etary energy density and energy intake, genes required for mitochondrial oxida- pants were taking antihypertensive med-
which are not fully compensated for by tive phosphorylation in skeletal muscle ications, which may have blunted the
increased food intake (16,17). Our data (21). In contrast, a case-control study effect of diet on blood pressure.
suggest that the weight-reducing effect of found that soleus muscle intramyocellu- In conclusion, in individuals with
the vegan diet (4) is responsible for a sub- lar lipid concentrations were significantly type 2 diabetes participating in a 22-week
stantial portion of its effect on A1C. lower in a group of 21 vegans compared clinical trial, both a low-fat vegan diet and
Independent of their effect on body with 25 omnivores (Ϫ9.7 [95% CI Ϫ16.2 a diet following ADA guidelines improved
weight, reductions in total fat intake and to Ϫ3.3], P ϭ 0.01) (22). glycemic control; however, the changes
in the proportion of dietary saturated to The lipid-lowering effect of vegan di- were greater in the vegan group. Further
unsaturated fat increase insulin sensitivity ets, attributable to their absence of dietary research is necessary to establish longer-
(18), as do increased intake of low– cholesterol, low saturated fat content, and term diet effects and sustainability.
glycemic index and high-fiber foods (1). a specific cholesterol-reducing effect of
Finally, limited evidence suggests soluble fiber and other plant constituents
that reductions in iron stores increase in- (23), is particularly important given that Acknowledgments — The study was sup-
sulin sensitivity (19). A vegan diet pro- cardiovascular complications are the pri- ported by grant R01 DK059362-01A2 from
vides iron in its nonheme form, which is mary cause of morbidity and mortality in the National Institute of Diabetes and Diges-
tive and Kidney Diseases and by the Diabetes
somewhat less absorbable than heme diabetes. While diets high in refined car- Action Research and Education Foundation.
iron. A study comparing 30 ovolactoveg- bohydrate may increase triglyceride con- The authors express appreciation to Paul
etarians and 30 meat eaters, all of whom centrations, high-fiber and low– glycemic Poppen, PhD, for statistical analyses.
were healthy and had BMIs Ͻ23 kg/m2, index foods appear to have the opposite
showed that vegetarians had adequate, result (24).
but lower, body iron stores, compared The limited compliance of the ADA References
with meat eaters (serum ferritin concen- group merits comment. Researchers have 1. Jenkins DJA, Kendall CWC, Marchie A,
tration 35 g/l [95% CI 21– 49] vs. 72 long lamented the difficulties in adhering Jenkins AL, Augustin LSA, Ludwig DS,
g/l [45–100]). The vegetarians also to diets for diabetes (25). The A1C reduc- Barnard ND, Anderson JW: Type 2 diabe-
demonstrated less insulin resistance tion observed in the ADA group was sim- tes and the vegetarian diet. Am J Clin Nutr
(steady-state plasma glucose concentra- ilar to that found in previous studies (26). 78:610S– 616S, 2003
tion 4.1 mmol/l [3.5–5.0] vs. 6.9 mmol/l A potential weakness of the ADA guide- 2. Fraser GE: Vegetarianism and obesity, hy-
pertension, diabetes, A comprehensive
and arthritis. In Diet,
[5.2–7.5], respectively) (19). lines is that they require portion size lim- Life Expectancy, and Chronic Disease. Ox-
Insulin resistance is related to lipid its for overweight individuals, and bibliography is
ford, U.K., Oxford University Press,
accumulation within muscle cells (in- limitations on saturated-fat intake are 2003, p. 129 –148 typical in scholarly
tramyocellular lipid), apparently due to a based on these limited energy intakes. In- 3. Nicholson AS, Sklar M, Barnard ND, Gore
publications
genetically based reduction in mitochon- dividuals who exceed their prescribed en- S, Sullivan R, Browning S: Toward im-
drial activity identifiable many years be- ergy intake limits with overly large proved management of NIDDM: a ran-
1782 DIABETES CARE, VOLUME 29, NUMBER 8, AUGUST 2006](https://image.slidesharecdn.com/vegan2annotated-120621110137-phpapp02/85/Scholarly-Article-6-320.jpg)
![Barnard and Associates
domized, controlled, pilot intervention density lipoprotein cholesterol in plasma phosphorylation in skeletal muscle. Dia-
using a low-fat, vegetarian diet. Prev Med without use of the preparative ultracentri- betes 54:1926 –1933, 2005
29:87–91, 1999 fuge. Clin Chem 18:499 –502, 1972 22. Goff LM, Bell JD, So PW, Dornhorst A,
4. Barnard ND, Scialli AR, Turner-McGrievy 13. Corcoran RM, Durnan SM: Albumin de- Frost GS: Veganism and its relationship
G, Lanou AJ, Glass J: The effects of a low- termination by a modified bromocresol with insulin resistance and intramyocel-
fat, plant-based dietary intervention on green method (Letter). Clin Chem 23: lular lipid. Eur J Clin Nutr 59:291–298,
body weight, metabolism, and insulin 765–766, 1977 2005
sensitivity. Am J Med 118:991–997, 2005 14. Bouchard C, Tremblay A, LeBlanc C, 23. Jenkins DJ, Kendall CW, Marchie A,
5. Wilson DH, Bogacz JP, Forsythe CM, Lortie G, Savard R, Theriault G: A method Faulkner DA, Wong JM, de Souza R,
Turk PJ, Lane TL, Gates RC, Brandt DR: to assess energy expenditure in children Emam A, Parker TL, Vidgen E, Lapsley
Fully automated assay of glycohemoglo- and adults. Am J Clin Nutr 37:461– 467,
KG, Trautwein EA, Josse RG, Leiter LA,
bin with the Abbott IMx analyzer: novel 1983
Connelly PW: Effects of a dietary portfolio
approaches for separation and detection. 15. Krentz AJ, Bailey CJ: Oral antidiabetic
Clin Chem 39:2090 –2097, 1993 agents: current role in type 2 diabetes on cholesterol-lowering foods vs lova-
6. American Diabetes Association: Evi- mellitus (Review). Drugs 65:385– 411, statin on serum lipids and C-reactive pro-
dence-based nutrition principles and rec- 2005 tein. JAMA 290:502–510, 2003
ommendations for the treatment and 16. Kendall A, Levitsky DA, Strupp BJ, Liss- 24. Jenkins DJ, Wolever TM, Kalmusky J,
prevention of diabetes and related com- ner L: Weight loss on a low-fat diet: con- Guidici S, Giordano C, Patten R, Wong
plications (Position Statement). Diabetes sequence of the imprecision of the control GS, Bird JN, Hall M, Buckley G, et al.:
Care 26 (Suppl. 1):S51–S61, 2003 of food intake in humans. Am J Clin Nutr Low-glycemic index diet in hyperlipid-
7. Schakel SF, Sievert YA, Buzzard IM: 53:1124 –1129, 1991 emia: use of traditional starchy foods.
Sources of data for developing and main- 17. Howarth NC, Saltzman E, Roberts SB: Di- Am J Clin Nutr 46:66 –71, 1987
taining a nutrient database. J Am Diet As- etary fiber and weight regulation (Re- 25. Laitinen JH, Ahola IE, Sarkkinen ES, Win-
soc 88:1268 –1271, 1988 view). Nutr Rev 59:129 –139, 2001 berg RL, Harmaakorpi-Iivonen PA, Uus-
8. Barthelmai W, Czok R: Enzymatic deter- 18. Lovejoy JC, Windhauser MM, Rood JC, itupa MI: Impact of intensified dietary
minations of glucose in the blood, cere- de la Bretonne JA: Effect of a controlled therapy on energy and nutrient intakes
brospinal fluid and urine. Klin Wochenschr high-fat versus low-fat diet on insulin sen- and fatty acid composition of serum lipids
40:585–589, 1962 [in German] sitivity and leptin levels in African-Amer- in patients with recently diagnosed non-
9. Allain CC, Poon LS, Chan CSG, Rich- ican and Caucasian women. Metabolism insulin-dependent diabetes mellitus. J Am
mond W, Fu PC: Enzymatic determina- 47:1520 –1524, 1998 Diet Assoc 93:276 –283, 1993
tion of total serum cholesterol. Clin Chem 19. Hua NW, Stoohs RA, Facchini FS: Low
26. Franz MJ, Splett PL, Monk A, Barry B,
20:470 – 475, 1974 iron status and enhanced insulin sensitiv-
McClain K, Weaver T, Upham P, Bergen-
10. Wieland H, Seidel D: A simple specific ity in lacto-ovo vegetarians. Br J Nutr 86:
method for precipitation of low density 515–519, 2001 stal R, Mazze RS: Cost-effectiveness of
lipoproteins. J Lipid Res 24:904 –909, 20. Petersen KF, Dufour S, Befroy D, Garcia medical nutrition therapy provided by di-
1983 R, Shulman GI: Impaired mitochondrial etitians for persons with non-insulin-de-
11. Finley PR, Schifman RB, Williams RJ, activity in the insulin-resistant offspring pendent diabetes mellitus. J Am Diet Assoc
Licht DA: Cholesterol in high-density li- of patients with type 2 diabetes. N Engl 95:1018 –1024, 1995
poprotein: use of Mg2ϩ/dextran sulfate J Med 350:664 – 671, 2004 27. Barnard ND, Scialli AR, Turner-McGrievy
in its enzymatic measurement. Clin Chem 21. Sparks LM, Xie H, Koza RA, Mynatt R, GM, Lanou AJ: Acceptability of a low-fat
24:931–933, 1978 Hulver MW, Bray GA, Smith SR: A high- vegan diet compares favorably to a step II
12. Friedewald WT, Levy RI, Fredrickson DS: fat diet coordinately downregulates genes diet in a randomized, controlled trial.
Estimation of the concentration of low- required for mitochondrial oxidative J Cardiopulm Rehabil 24:229 –235, 2004
DIABETES CARE, VOLUME 29, NUMBER 8, AUGUST 2006 1783](https://image.slidesharecdn.com/vegan2annotated-120621110137-phpapp02/85/Scholarly-Article-7-320.jpg)











































































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)