Downloaded 45 times







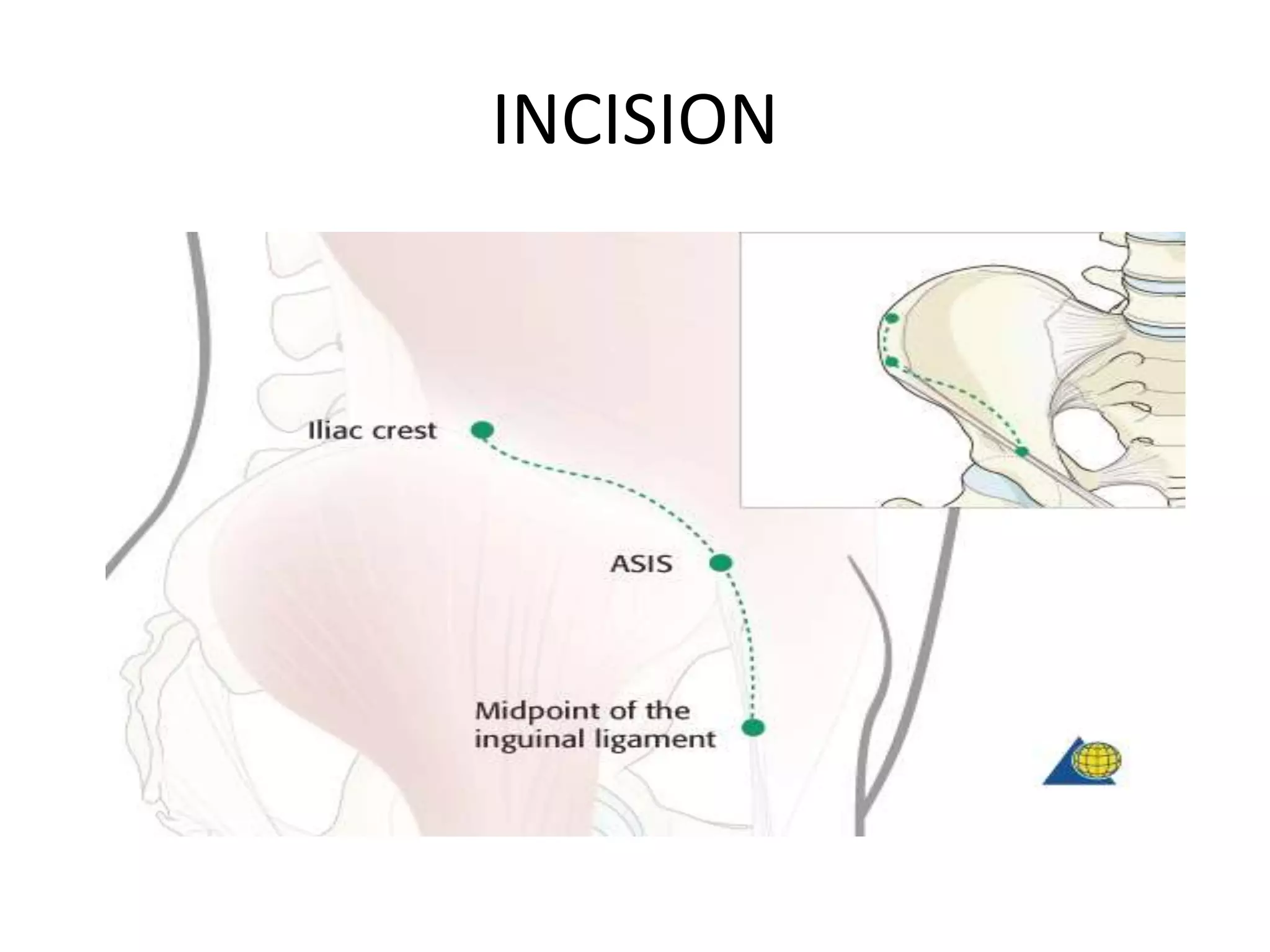


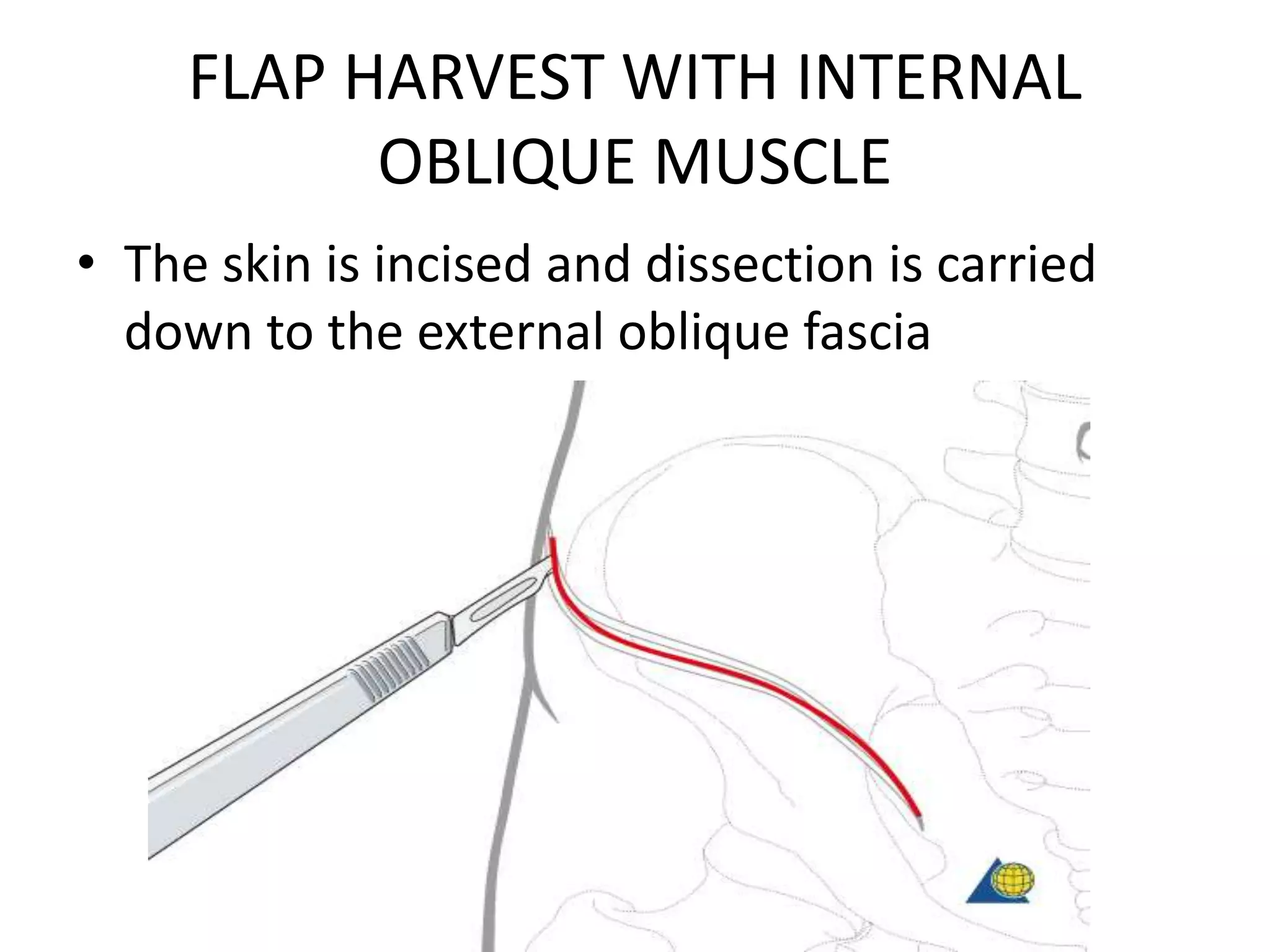
























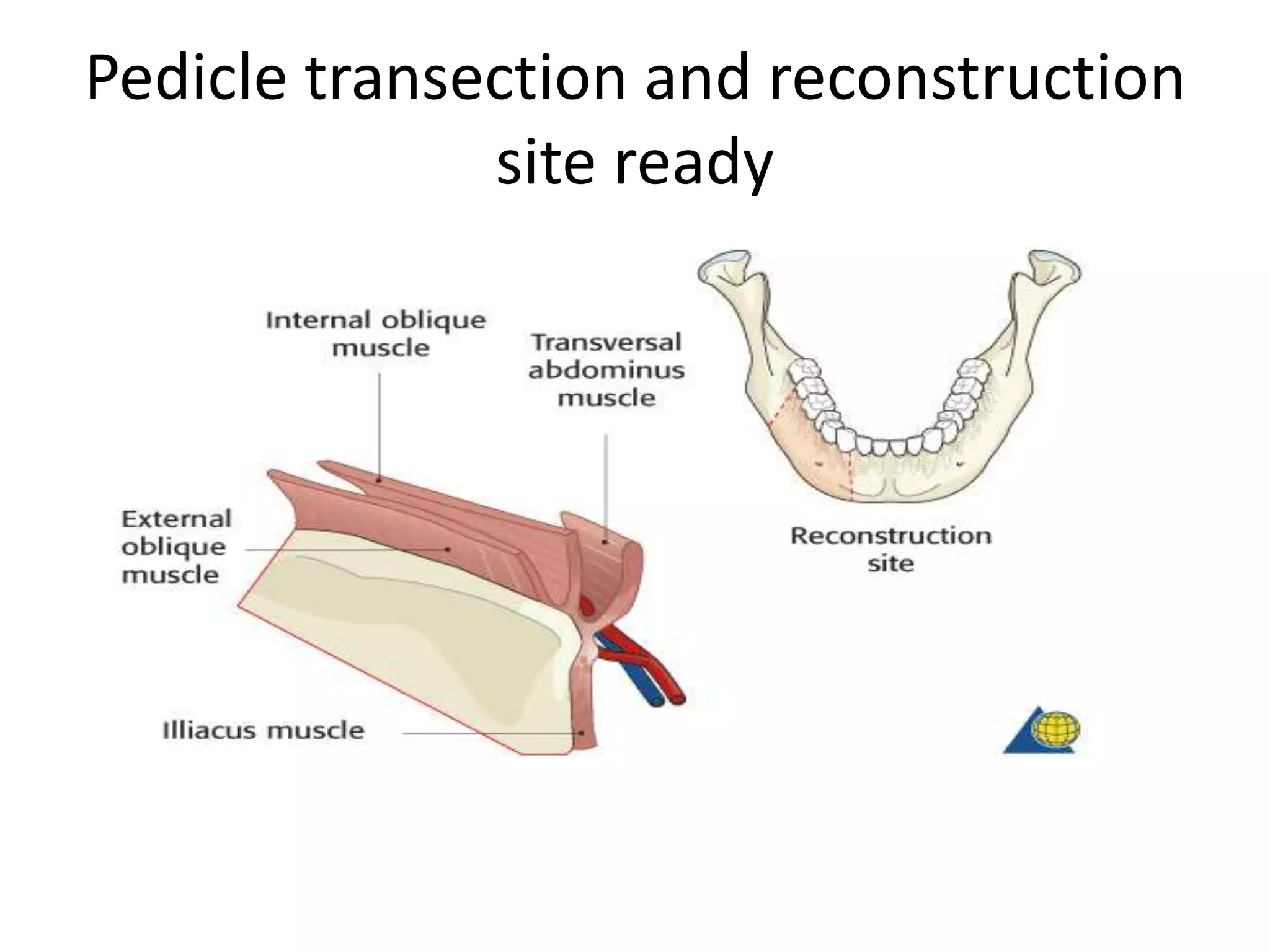









The document describes the anatomy and surgical technique for harvesting a deep circumflex iliac artery (DCIA) flap. The DCIA flap can include bone from the iliac crest and either the internal oblique muscle or just the overlying muscles. The standard incision is an S-shaped incision over the iliac crest. Dissection proceeds through the muscle layers to identify the DCIA and its branches. The flap is then harvested by ligating the DCIA, performing osteotomies, and transecting the pedicle once the reconstruction site is ready. Closure involves reapproximating the muscles and skin.























































































