Download as PDF, PPTX


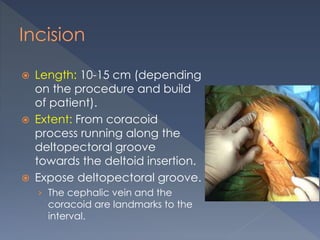
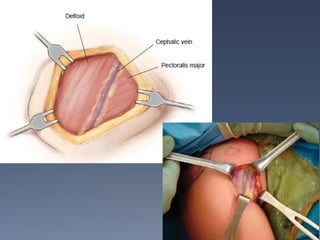
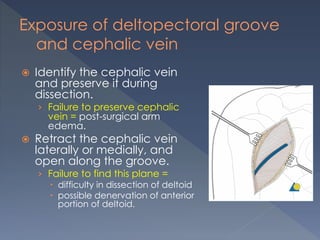
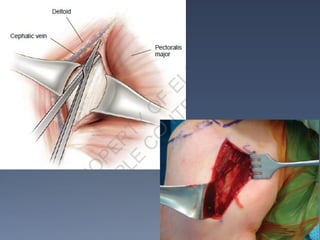
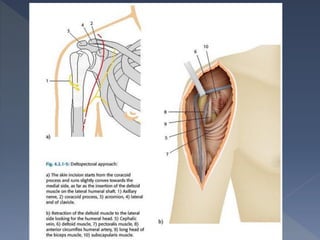
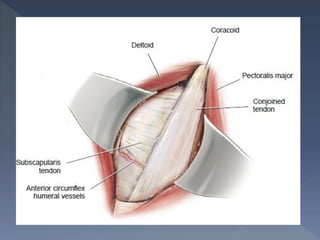



The anterior deltopectoral approach is used for various shoulder surgeries and fractures. It provides exposure of the shoulder joint and proximal humerus. The key steps are to identify the deltopectoral groove, preserve the cephalic vein, and laterally reflect the anterior deltoid. This exposes the coracoid process, joint capsule, tuberosities, and humeral head for procedures like shoulder arthroplasty and plating of humeral fractures. Care must be taken to protect structures like the axillary nerve and musculocutaneous nerve.













































































