Downloaded 120 times




















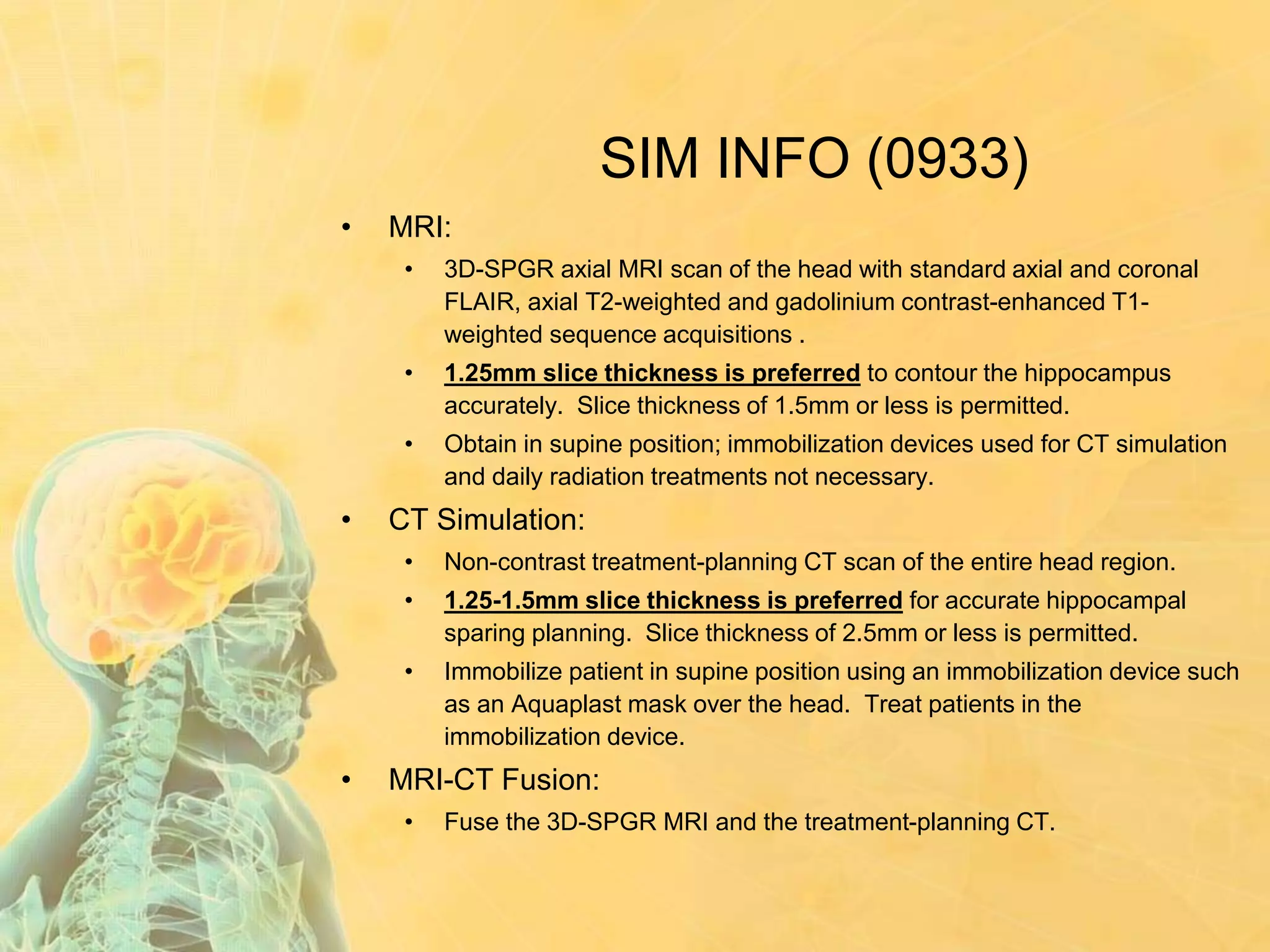
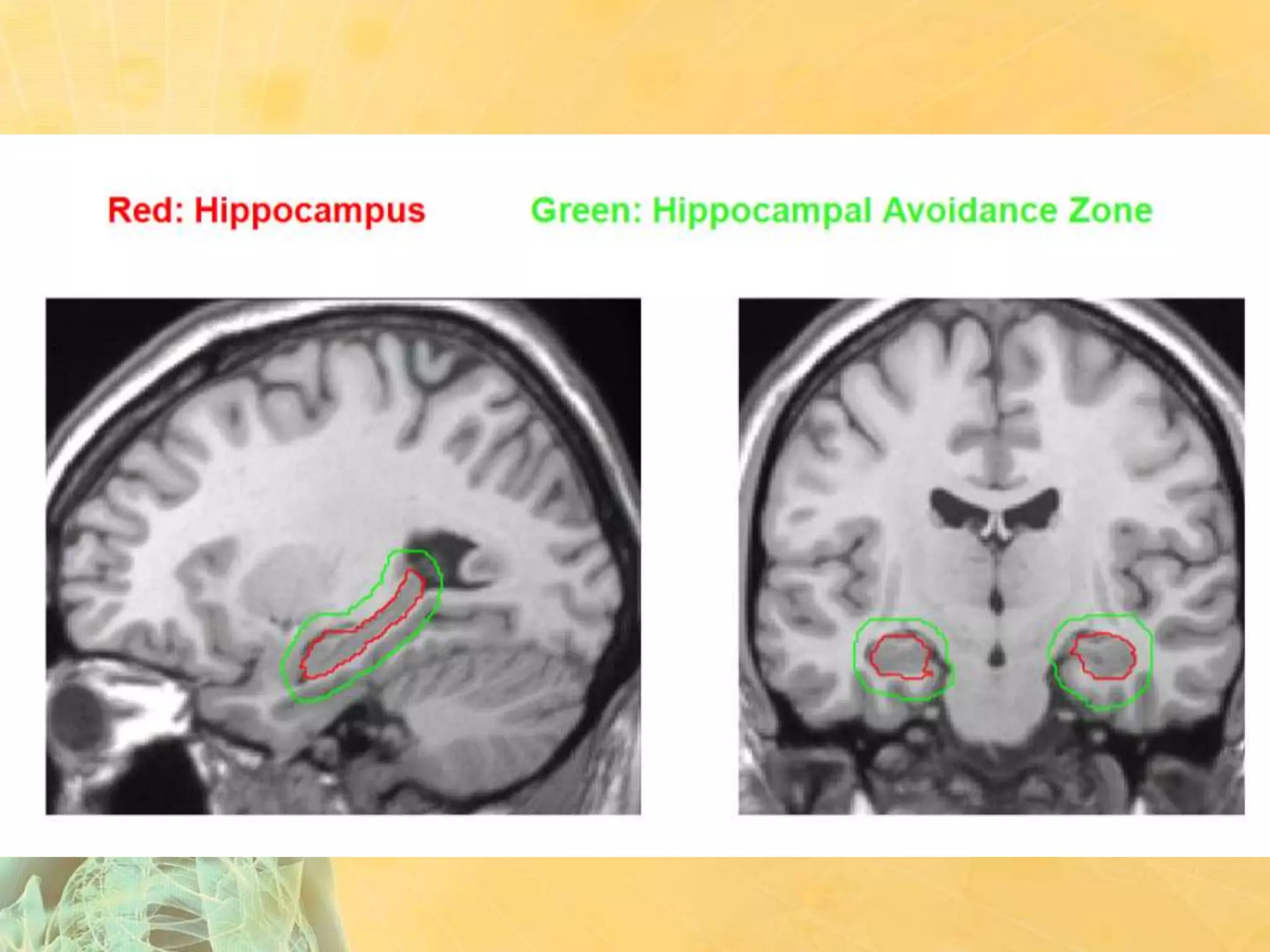


















- A 58-year-old female nurse presented with headache, nausea, and mental status changes. Imaging showed 3 brain metastases with no known primary site. - She had a KPS of 90, age <60, controlled primary (pending further workup), and no extracranial mets, placing her in RPA class I and GPA group with a predicted median survival of 7.1-11.3 months. - Treatment options included WBRT alone or WBRT with boost to reduce risk of neurocognitive toxicity based on the RTOG 0933 trial, which showed reduced memory decline with hippocampal avoidance. Patient selection focused on tumor types likely to benefit and survival duration to gain























































































