Hypofractionation in Prostate Cancer: Is Less Enough?
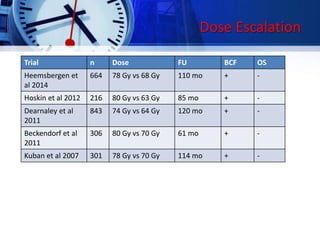
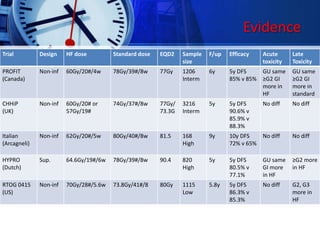
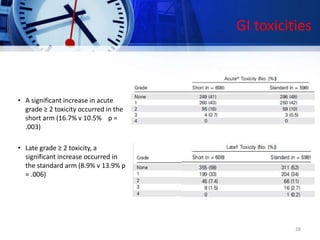
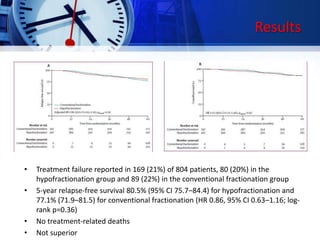
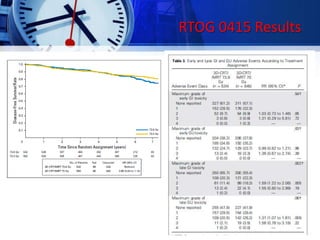
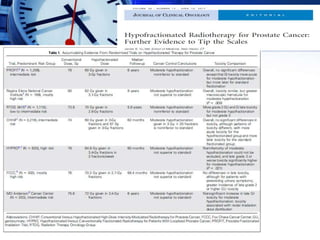
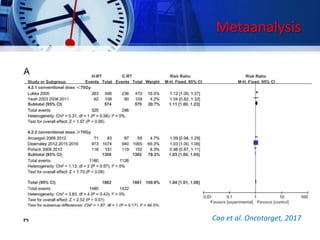
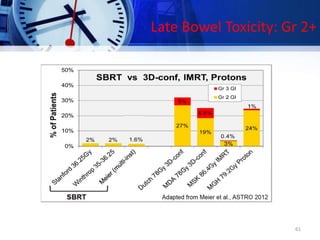
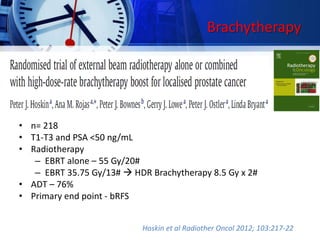
1) The document discusses several studies that have compared hypofractionated radiation therapy (delivering larger doses of radiation in fewer treatments) to standard fractionation for prostate cancer. The PROFIT trial found equivalent 5-year outcomes for intermediate risk prostate cancer patients treated with either 60Gy in 20 fractions over 4 weeks or 78Gy in 39 fractions over 7-8 weeks, with less late gastrointestinal toxicity in the hypofractionated group.
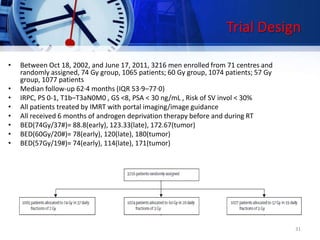
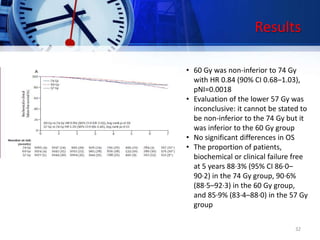
2) The CHHiP trial also found non-inferior 5-year outcomes when comparing 60Gy in 20 fractions to 74Gy in 37 fractions for intermediate risk prostate cancer, with no difference in toxicity.


![Roach formulas
• Partin’s risk nomograms uses pretreatment PSA,
Gleason score, and T category for risk assessment.
• Seminal vesicle involvement - PSA +([GS-6] x 10)
– Cutoff is 13%
– If <13%, risk 7%; if >=13%, risk 37%.
• Lymph node involvement - 2/3 x PSA + ([GS-6] x 10)
– Cutoff is 15%.
– If calculated risk is <15%, actual risk 6%; if >=15%,
actual risk 40%.
• Extracapsular extension - 3/2 x PSA + ([GS-3) x 10)
– Approximates actual risk
10](https://image.slidesharecdn.com/finalseminarhypoinprostate-170901144152/85/Hypofractionation-in-carcinoma-prostate-10-320.jpg)

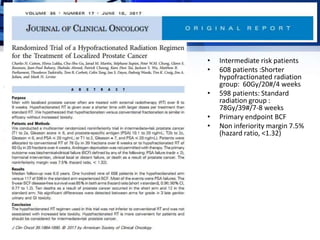
![• Lee et al, JCO April 2016(US based)
• 1,115 men with low-risk prostate cancer (T1b to T2c,GS 2-6, PSA<10)
• C-RT (73.8 Gy/41#/8.2 wks) 1.8gy/# vs
• H-RT (70 Gy/28#/5.6 wks) 2.5Gy/#
• Median follow-up 5.8 years
• Trial designed to establish (with 90% power and an alpha of .05) that
treatment with H-RT results in 5-year disease-free survival (DFS) that is
not worse than C-RT by more than 7.65% (H-RT/C-RT hazard ratio [HR] ,
1.52
• BED (H-RT): Tumor=186.67, Early = 87.5, Late = 128.33
• BER (C-RT): Tumor= 162.36, Early = 87.08, Late = 118
41
RTOG 0415 Trial design](https://image.slidesharecdn.com/finalseminarhypoinprostate-170901144152/85/Hypofractionation-in-carcinoma-prostate-41-320.jpg)





















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
















