Downloaded 39 times




































![• NAME
• UMR
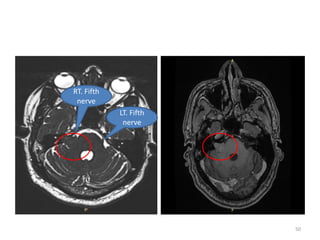
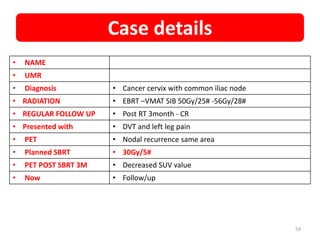
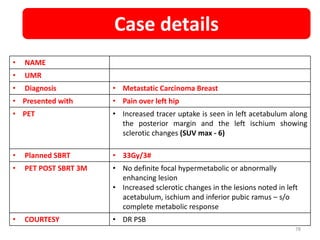
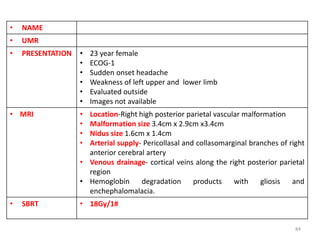
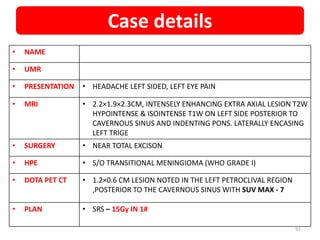
• PRESENTATION • Headache, difficulty in swallowing, Hoarseness of voice, Tinnitus
, reduced hearing, Nasal regurgitation × 6 months
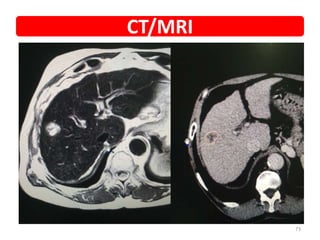
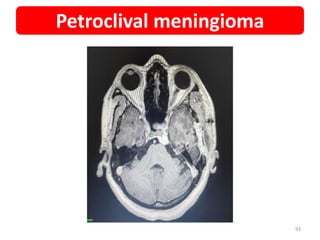
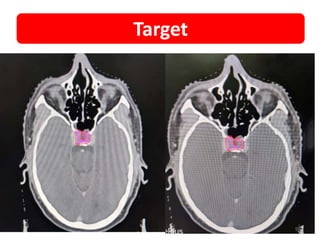
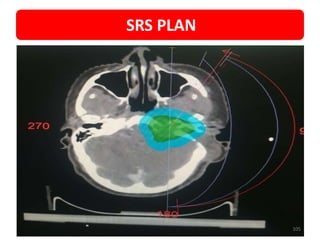
• MRI • 2.5 x2 cm, Brilliantly enhancing, extracranial lesion in Left jugular
foramen
• Hypo on T1 and Iso on T2
• Erosion of carotid canal and jugular foramen
• SURGERY • Excision of Glomus jugulare done by FISCH type approach
• BIOPSY • well defined nests separated by highly vascularized fibrous
septae[zelle ballen pattern]
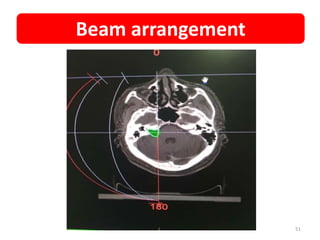
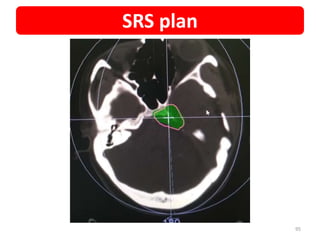
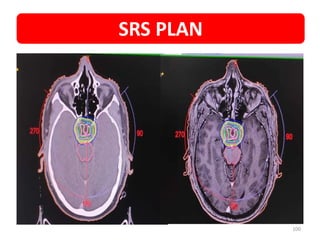
• SRS • 14Gy/1#
• IHC • Synaptophysin positive
• S100 positive
• COURTESY • DR PSB
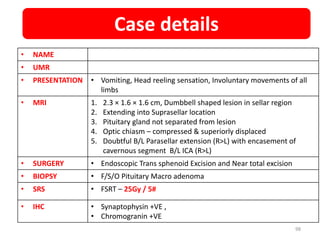
Case details
103](https://image.slidesharecdn.com/oursrsexperience-210416150200/85/STEREOTAXY-EXPERIENCE-SRS-SBRT-103-320.jpg)








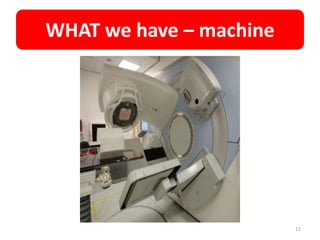
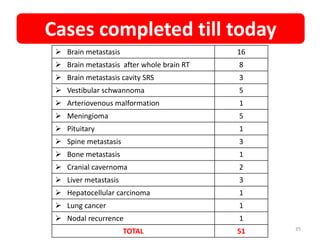
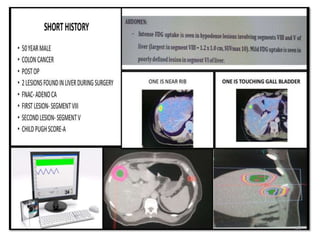
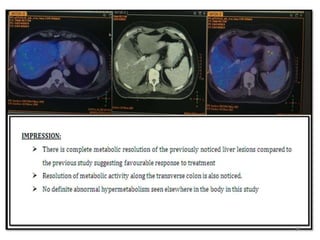
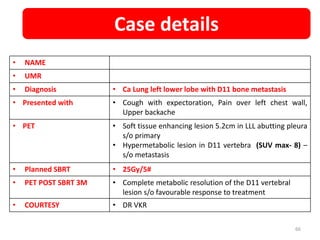
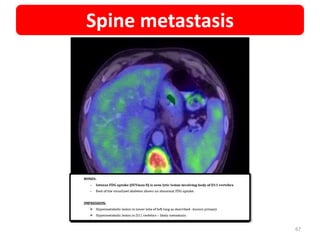
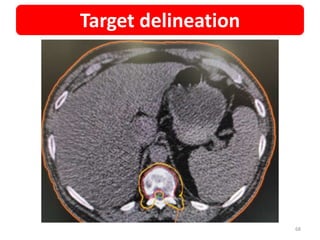
SRS/SBRT experience at Maharaja Gandhi Cancer Hospital for the first 50 cases: - SRS/SBRT uses precisely focused radiation beams to treat tumors with high doses in a single or few fractions while avoiding damage to surrounding tissue. - Their experience includes cranial and extracranial tumors treated with SRS and SBRT such as brain metastases, meningiomas, pituitary tumors, and tumors in the liver, spine, and lymph nodes. - Outcomes have been good with response seen on follow up imaging for various tumors including metabolic/structural resolution of treated lesions. - The hospital is well equipped for SRS/SBRT with a dedicated machine, immobil























































































