Downloaded 13 times
![Analysis 1.2. Comparison 1 Whole-Brain Radiotherapy versus Observation, Outcome 2 Progression Free
Survival.
Review: Surgery or radiosurgery plus whole brain radiotherapy versus surgery or radiosurgery alone for brain metastases
Comparison: 1 Whole-Brain Radiotherapy versus Observation
Outcome: 2 Progression Free Survival
Study or subgroup
Whole-Brain
Radiotherapy Observation log [Hazard Ratio] Hazard Ratio Weight Hazard Ratio
N N (SE) IV,Random,95% CI IV,Random,95% CI
Kocher 2011 180 179 -0.34 (0.11) 88.4 % 0.71 [ 0.57, 0.88 ]
Roos 2006 10 9 0.24 (0.52) 11.6 % 1.27 [ 0.46, 3.52 ]
Total (95% CI) 190 188 100.0 % 0.76 [ 0.53, 1.10 ]
Heterogeneity: Tau2 = 0.03; Chi2 = 1.19, df = 1 (P = 0.28); I2 =16%
Test for overall effect: Z = 1.47 (P = 0.14)
Test for subgroup differences: Not applicable
0.5 0.7 1 1.5 2
Favours WBRT Favours Observation
Soon et al, Cochrene metaanalysis, 2014
Brain metastasis: Cochrane meta-analysis 2014
Surgery/SRS+ WBRT Vs SRS/Surgery alone: Progression free Survival
WBRT: Definite reduction in local failure
p-value=0..14](https://image.slidesharecdn.com/srsdebate-dr-170703072707/85/Srs-debate-dr-ashutosh-mukherji-7-320.jpg)
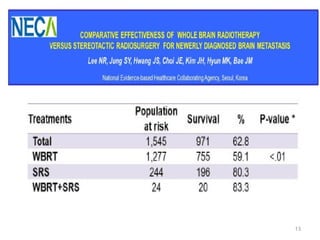
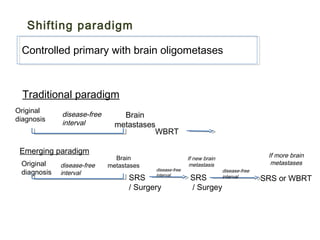
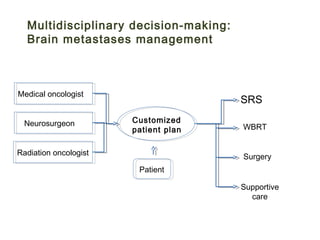
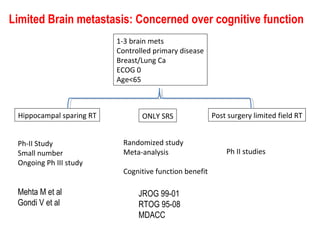
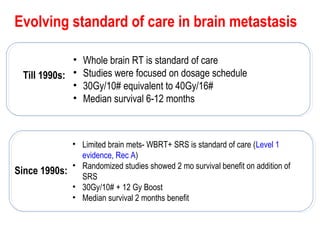


The document discusses treatment options for brain metastases including surgery, whole brain radiation therapy (WBRT), and stereotactic radiosurgery (SRS). It notes that while WBRT was traditionally used, studies show SRS alone may be preferred for limited brain metastases to avoid cognitive decline risks from WBRT. For larger or multiple tumors, WBRT provides better local and distant tumor control compared to SRS alone. Ongoing research evaluates hippocampal-sparing WBRT and the role of SRS boost after surgery to improve outcomes while preserving cognition. The optimal approach depends on disease factors and emerging evidence favors SRS for limited metastases to balance survival benefits with quality of life.


















































































