Download as PDF, PPTX






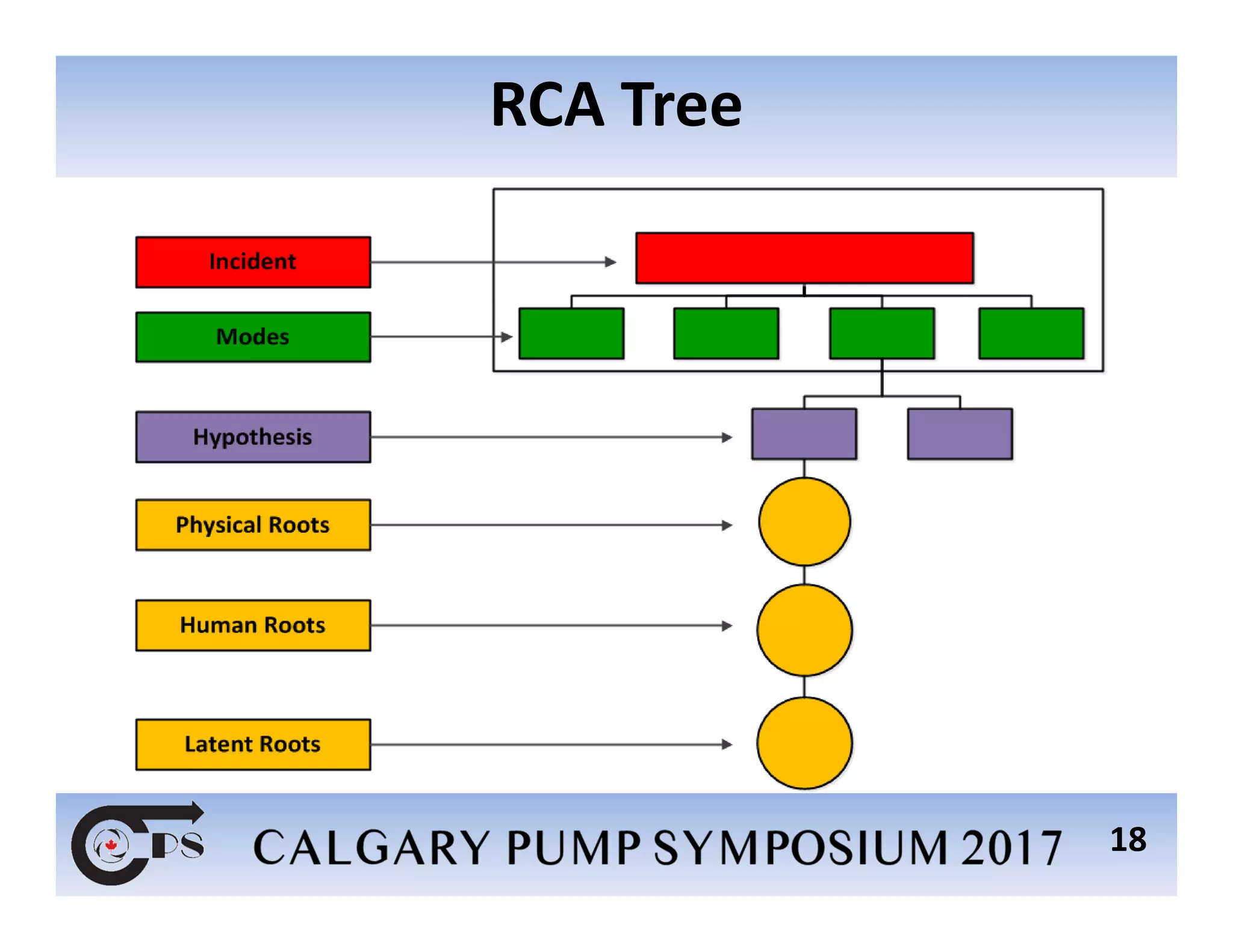
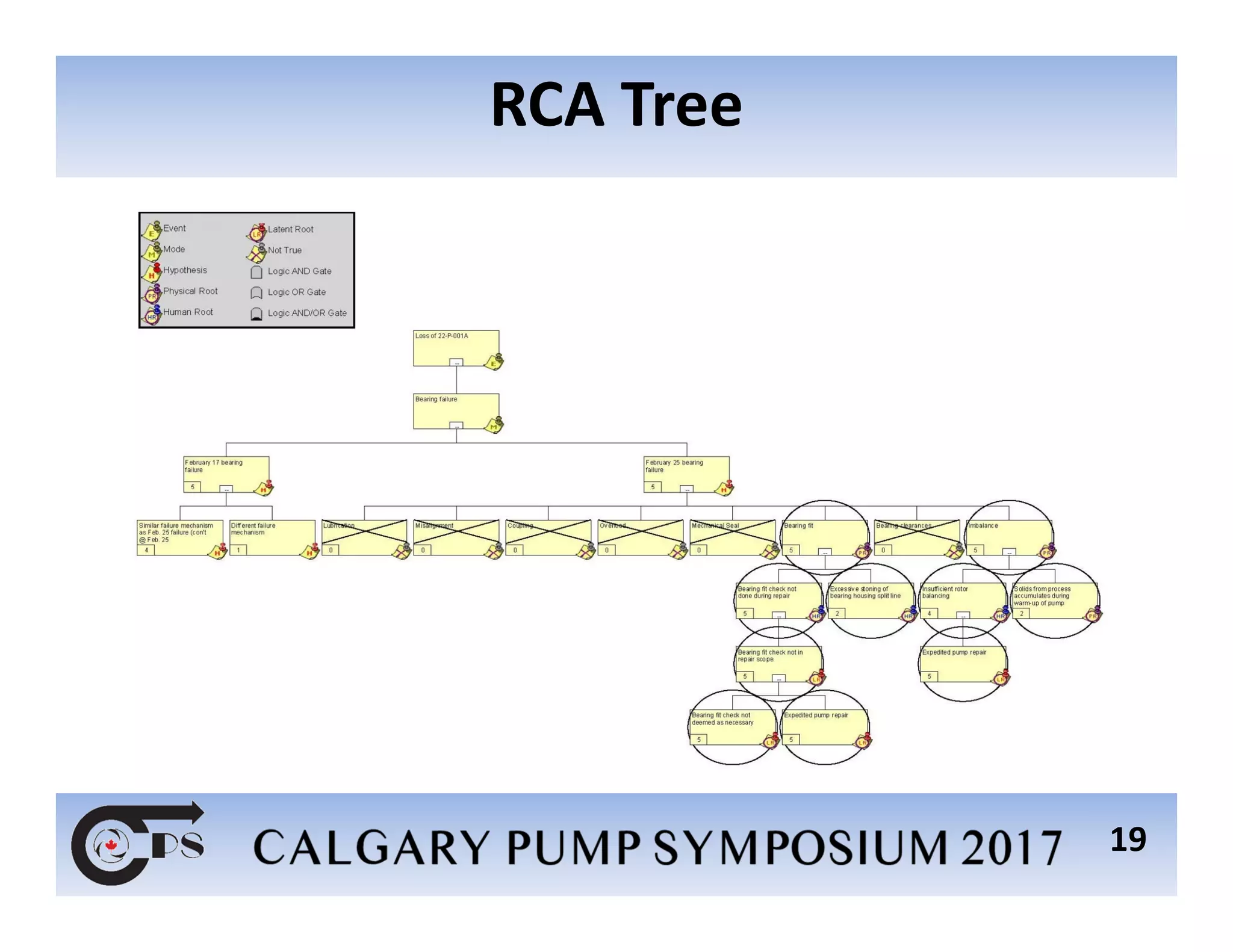
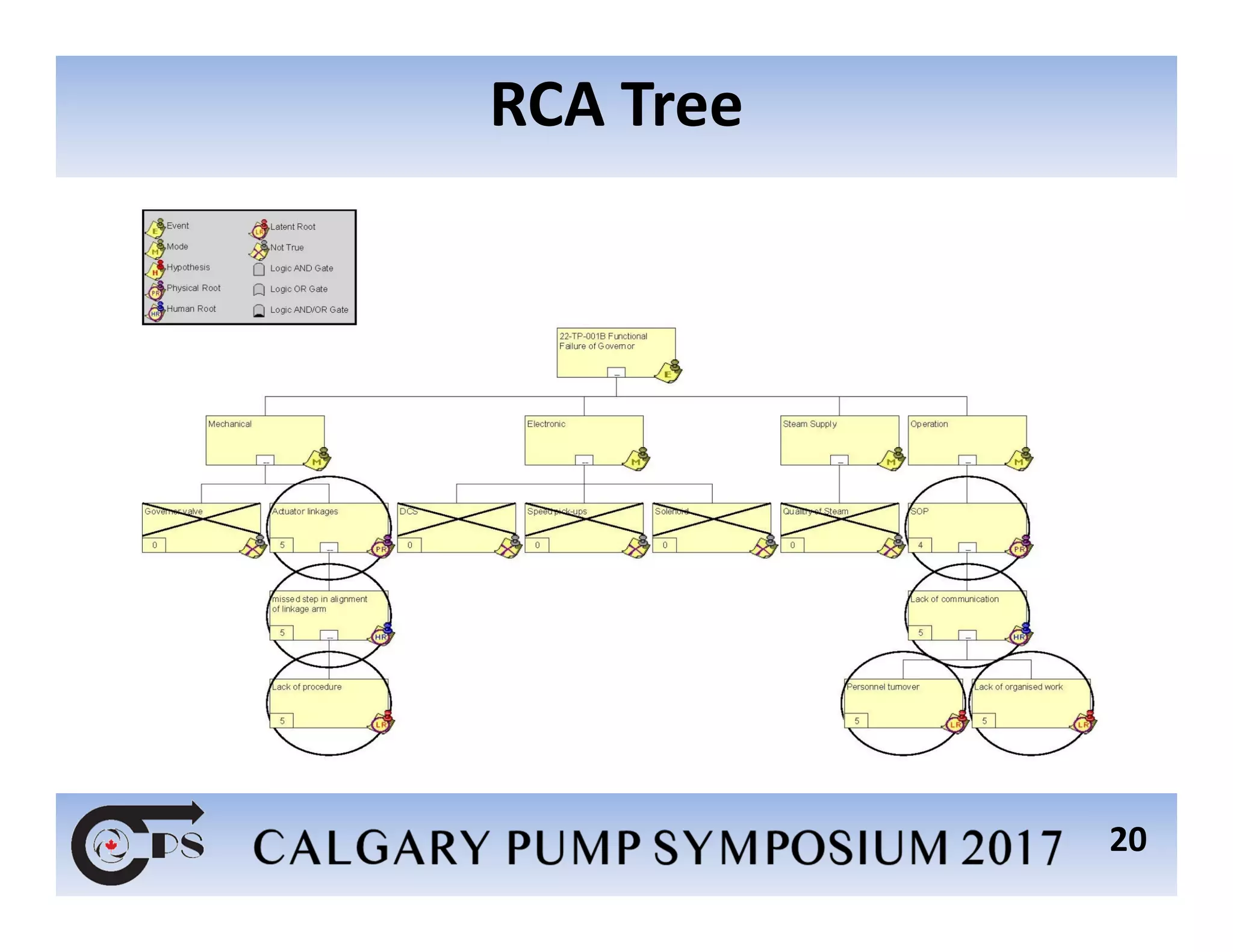
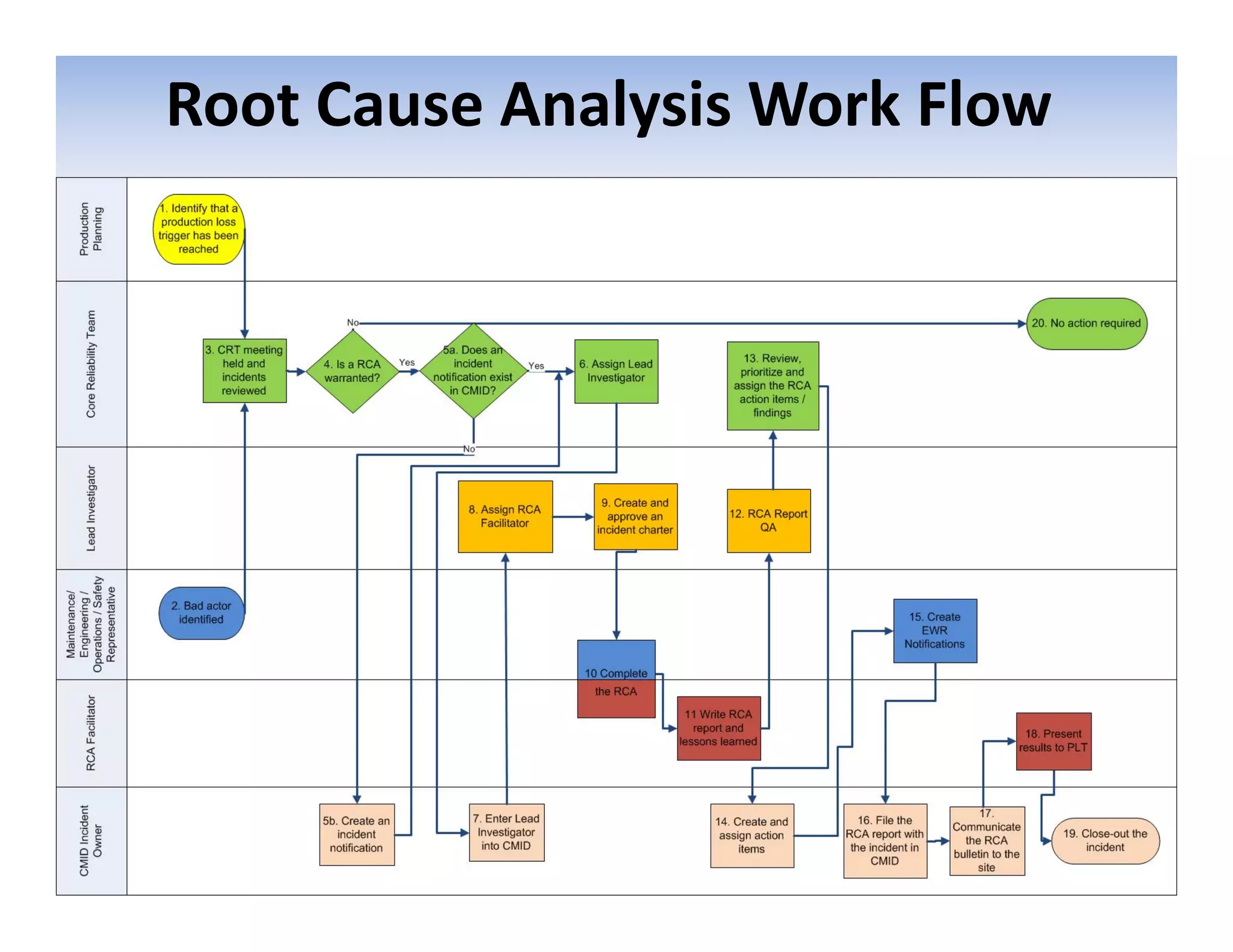













This document discusses root cause analysis methodology for troubleshooting pump failures. It begins by defining key terms like incident, root cause, and root cause analysis. It then outlines the root cause analysis process, which involves preserving event information, assembling an analysis team, analyzing to identify physical, human, and latent roots, communicating findings and recommendations, and tracking results. Common root causes are discussed. The document concludes by presenting two case studies where root cause analysis was used to troubleshoot pump issues and identify underlying causes.















































































