Downloaded 1,069 times
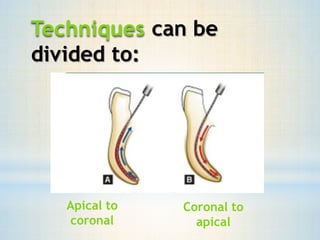
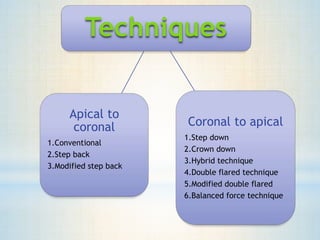



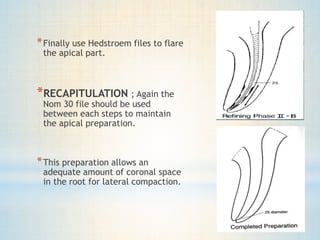











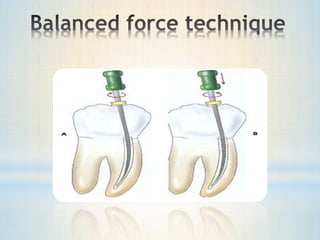




This document discusses various root canal preparation techniques including step-back, crown-down, and balanced force techniques. It provides details on each technique's procedures, advantages, and limitations. The step-back technique involves initial apical preparation followed by step-wise coronal preparation to create tapers. Crown-down starts with coronal flaring before apical instrumentation to minimize debris extrusion. Hybrid and balanced force techniques combine aspects of different methods.





















































































