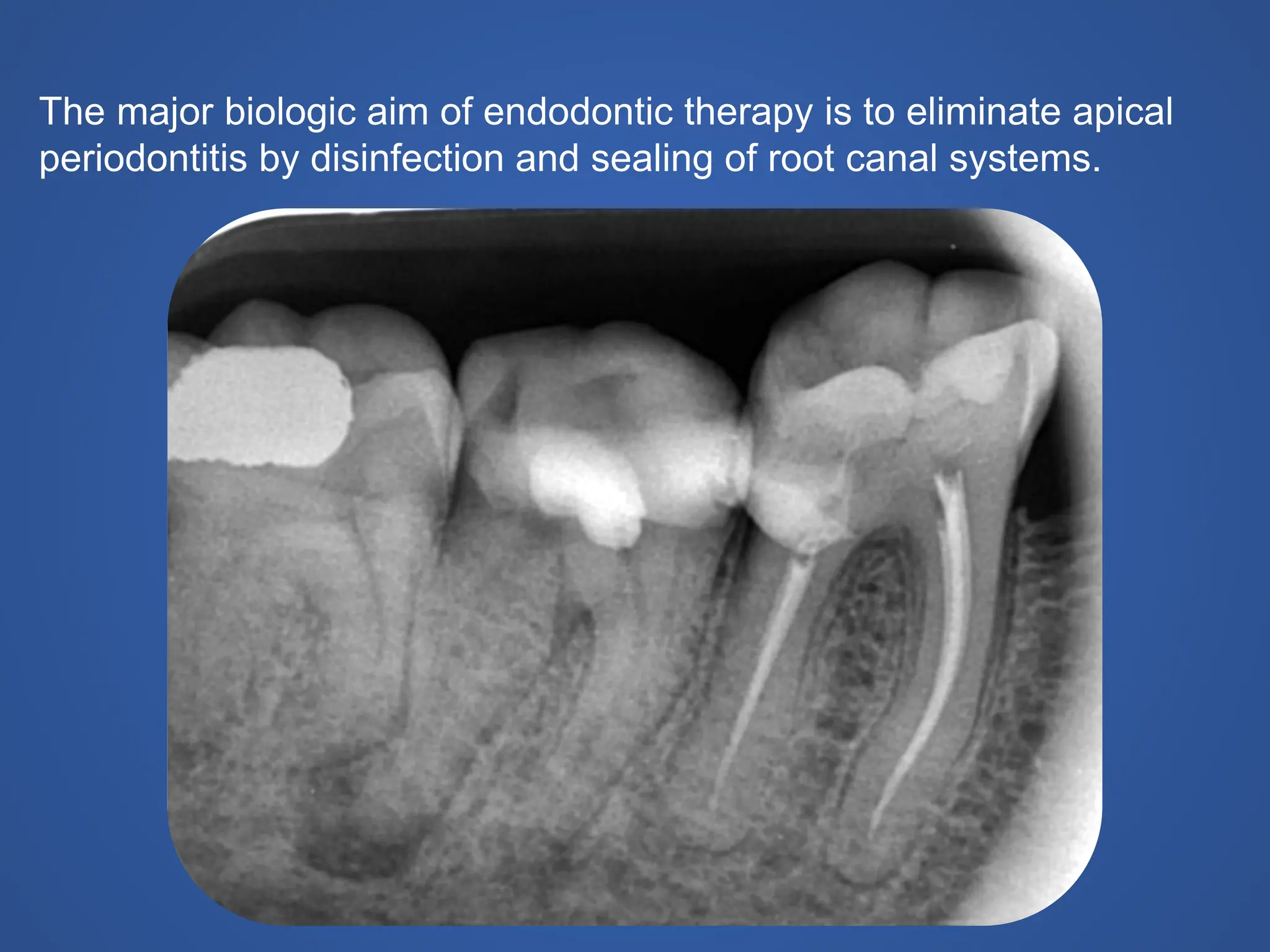
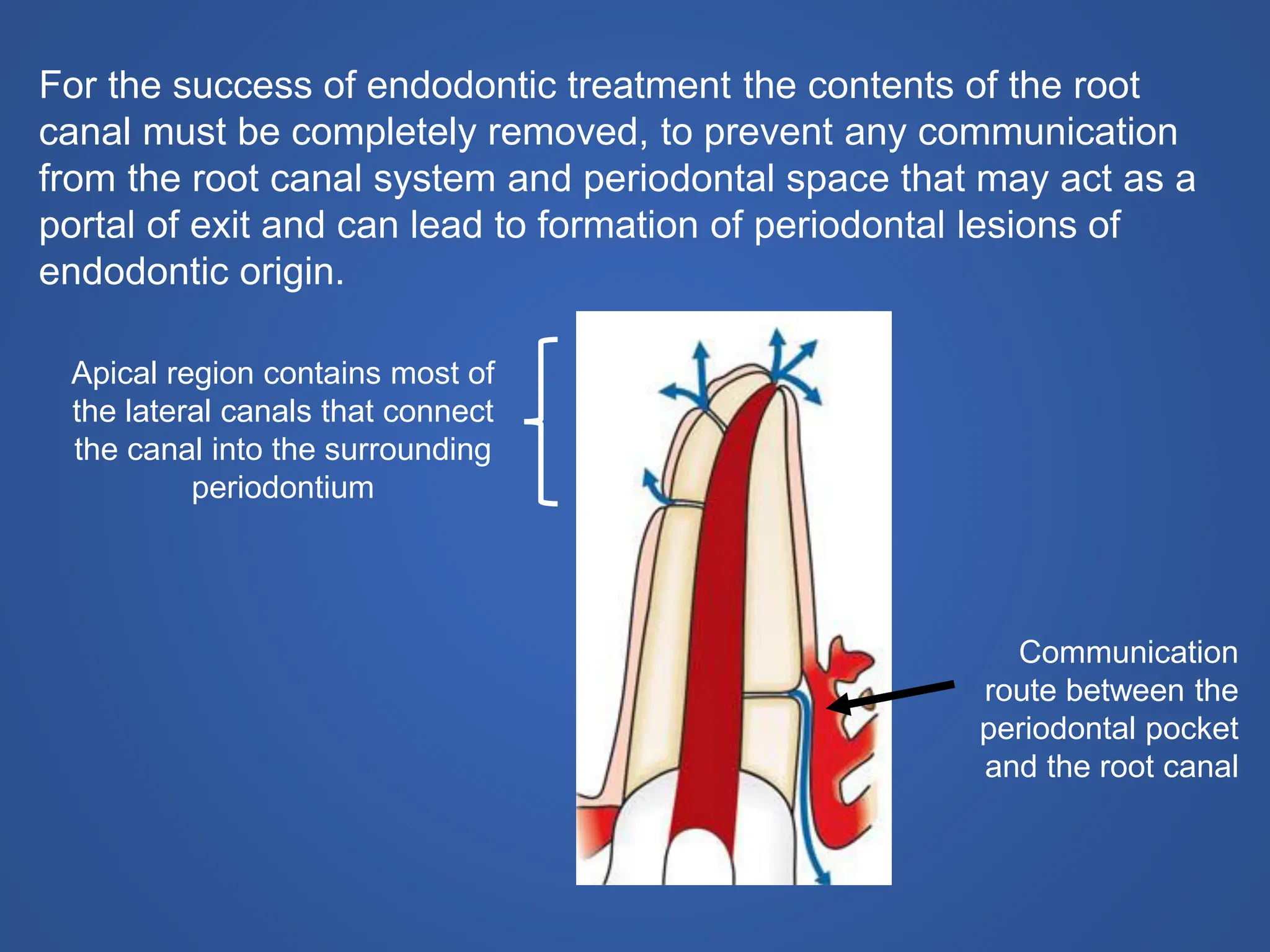
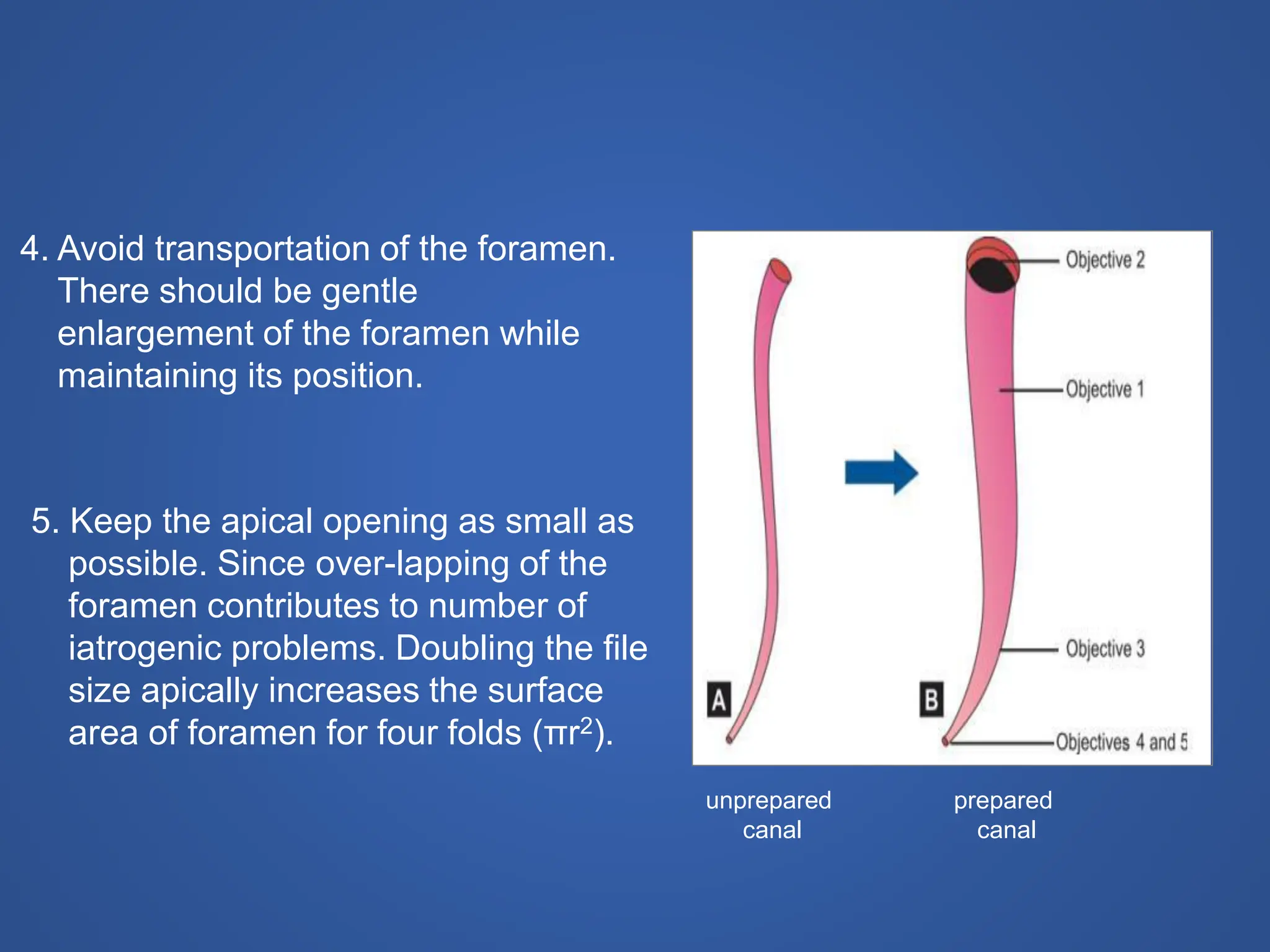
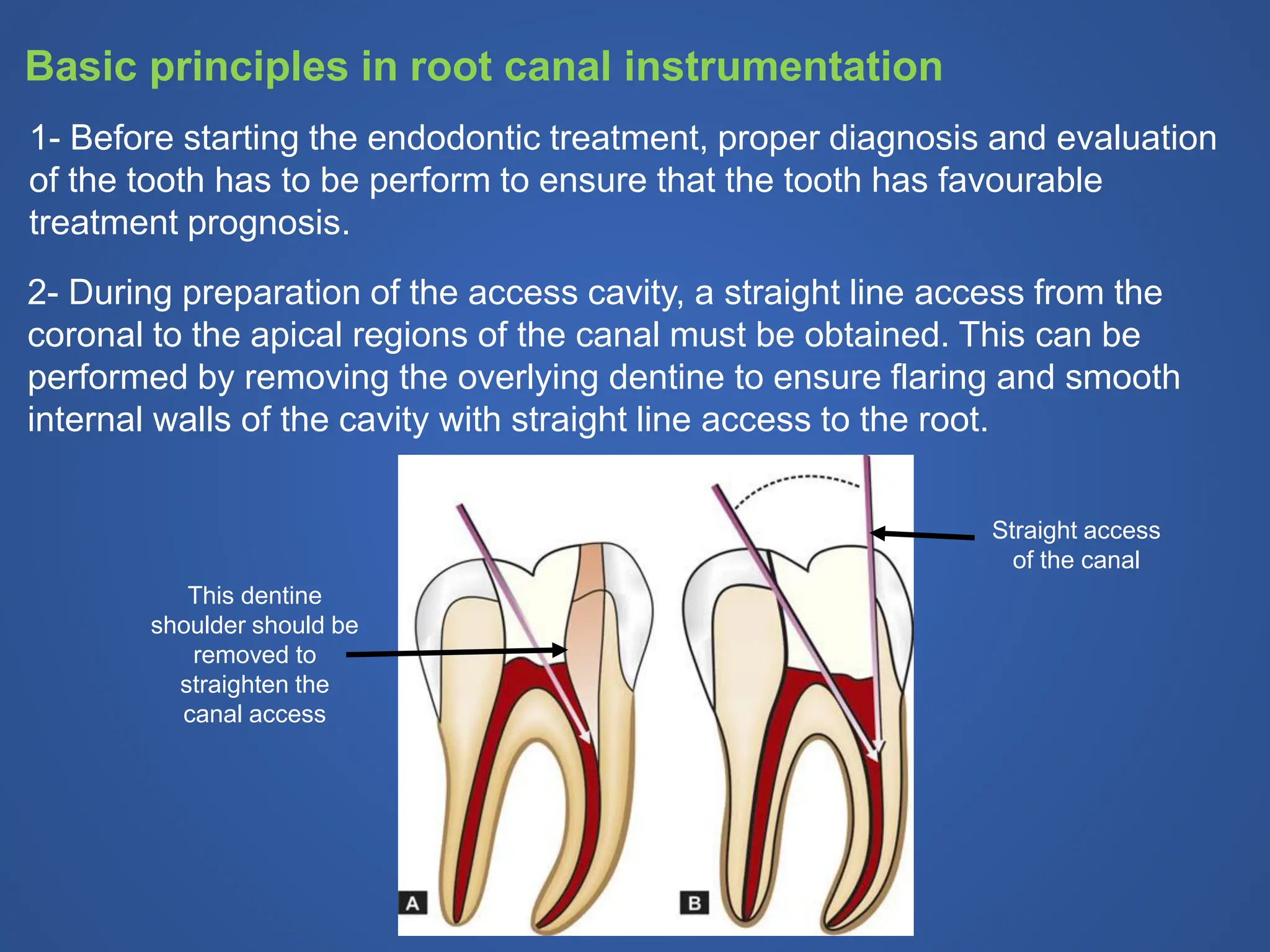
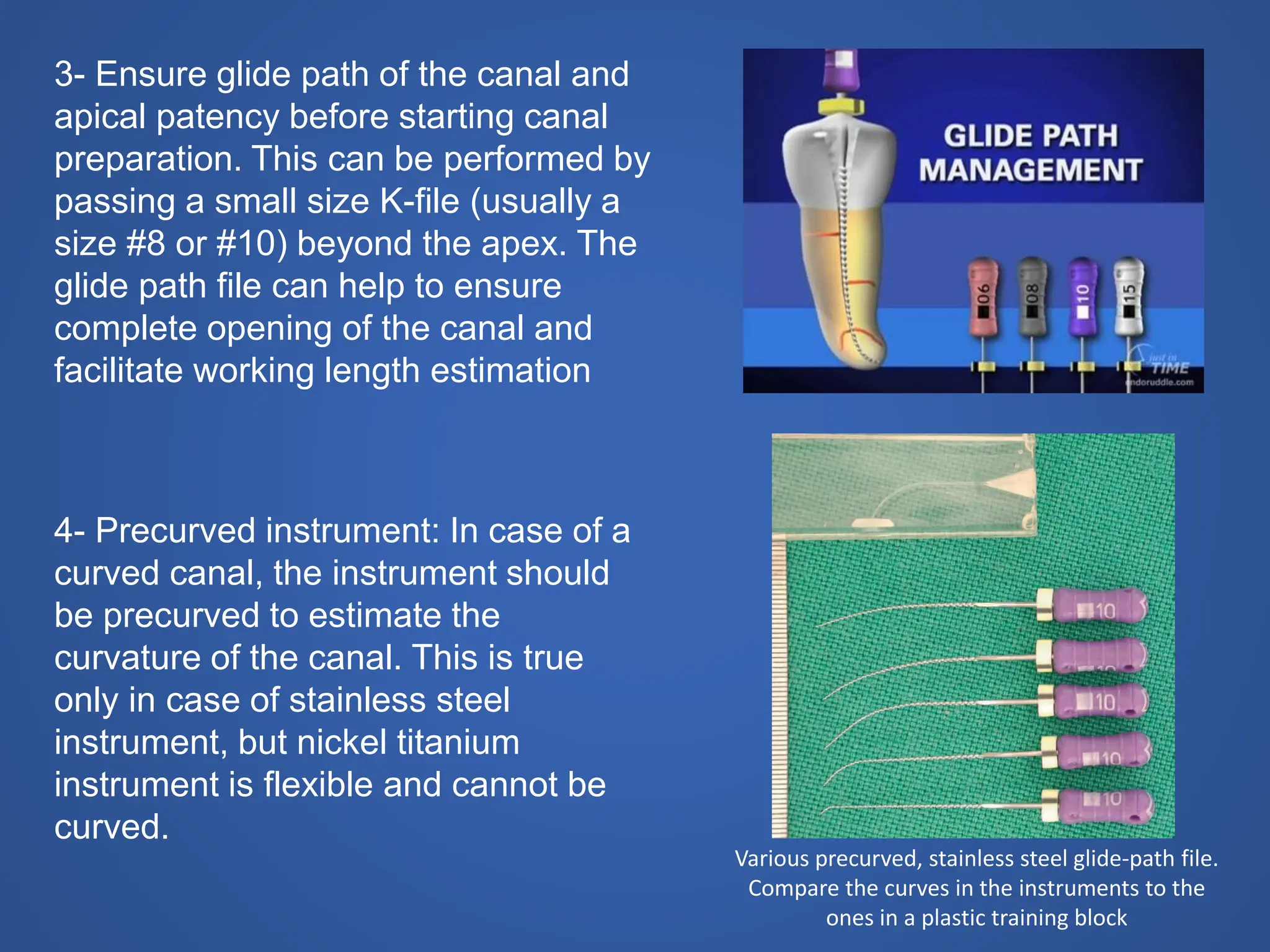
The document discusses cleaning and shaping of the root canal, which involves removing potentially pathogenic contents from the root canal system through cleaning, and establishing a tapered shape through the canal to allow for obturation. It outlines the objectives of endodontic treatment, and explains that cleaning and shaping is an important step to eliminate apical periodontitis by disinfecting and sealing the root canal. The principles of root canal instrumentation are also described, including maintaining the original shape of the canal, using irrigation, and preparing the canal in a gradual, sequential manner from small to large instruments to ensure the apical foramen is not over-enlarged.