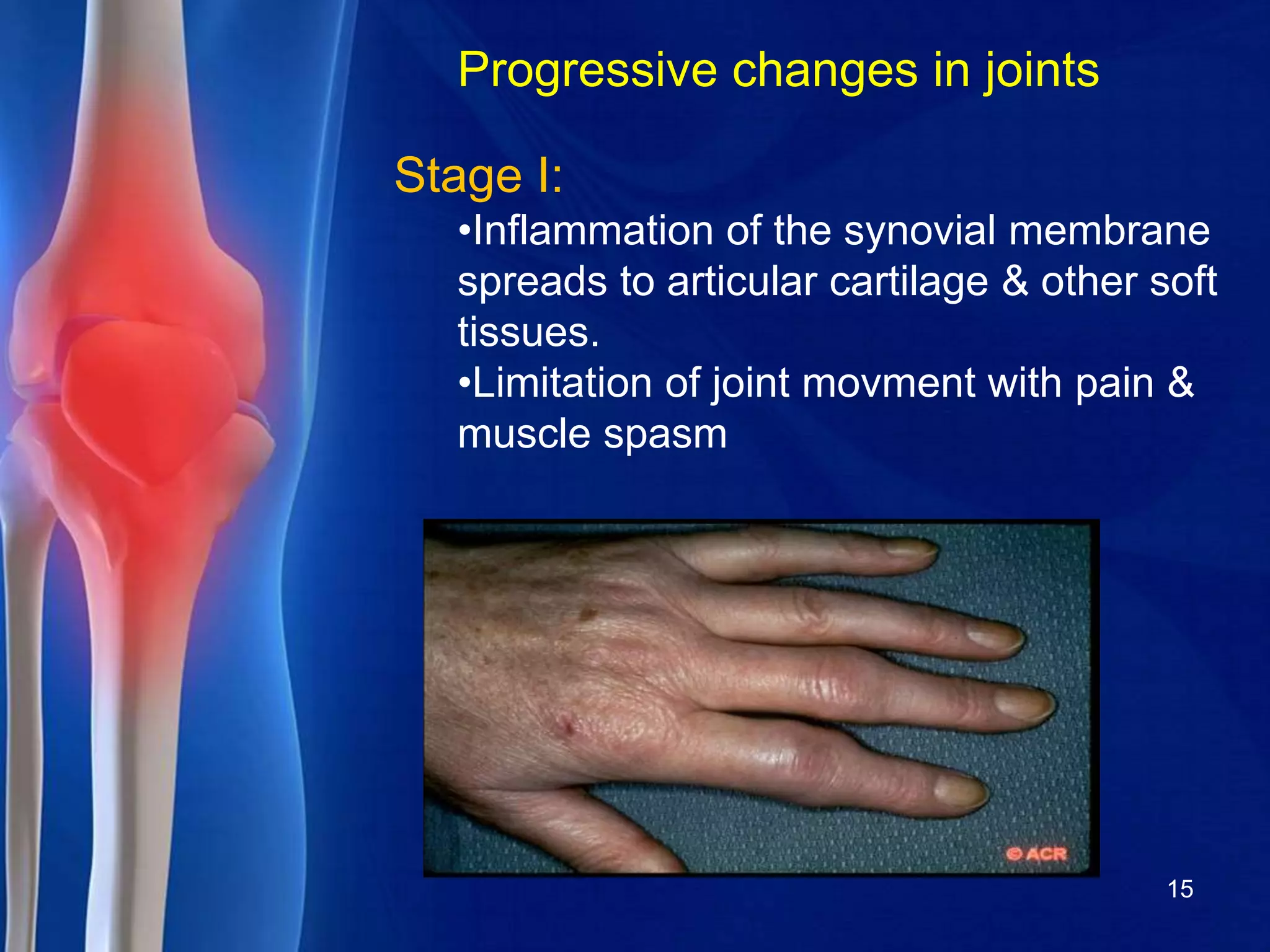
Rheumatoid arthritis is a chronic autoimmune disease that causes inflammation of the joints. It affects around 1% of the global population and is three times more common in women than men. While the exact cause is unknown, genetic and environmental factors are believed to play a role. RA results in painful swelling of the joints, stiffness, and over time can cause permanent joint damage and deformity. Diagnosis involves physical exam, blood tests to check for inflammatory markers and autoantibodies, and x-rays. Treatment aims to reduce inflammation and prevent further joint damage through medications, exercise, and assistive devices. While there is no cure, early and aggressive treatment can help control symptoms and minimize disability.












![1987 AMERICAN COLLEGE OF RHEUMATOLOGY
CRITERIA FOR RA
• Patients must have 4 of the 7 criteria:
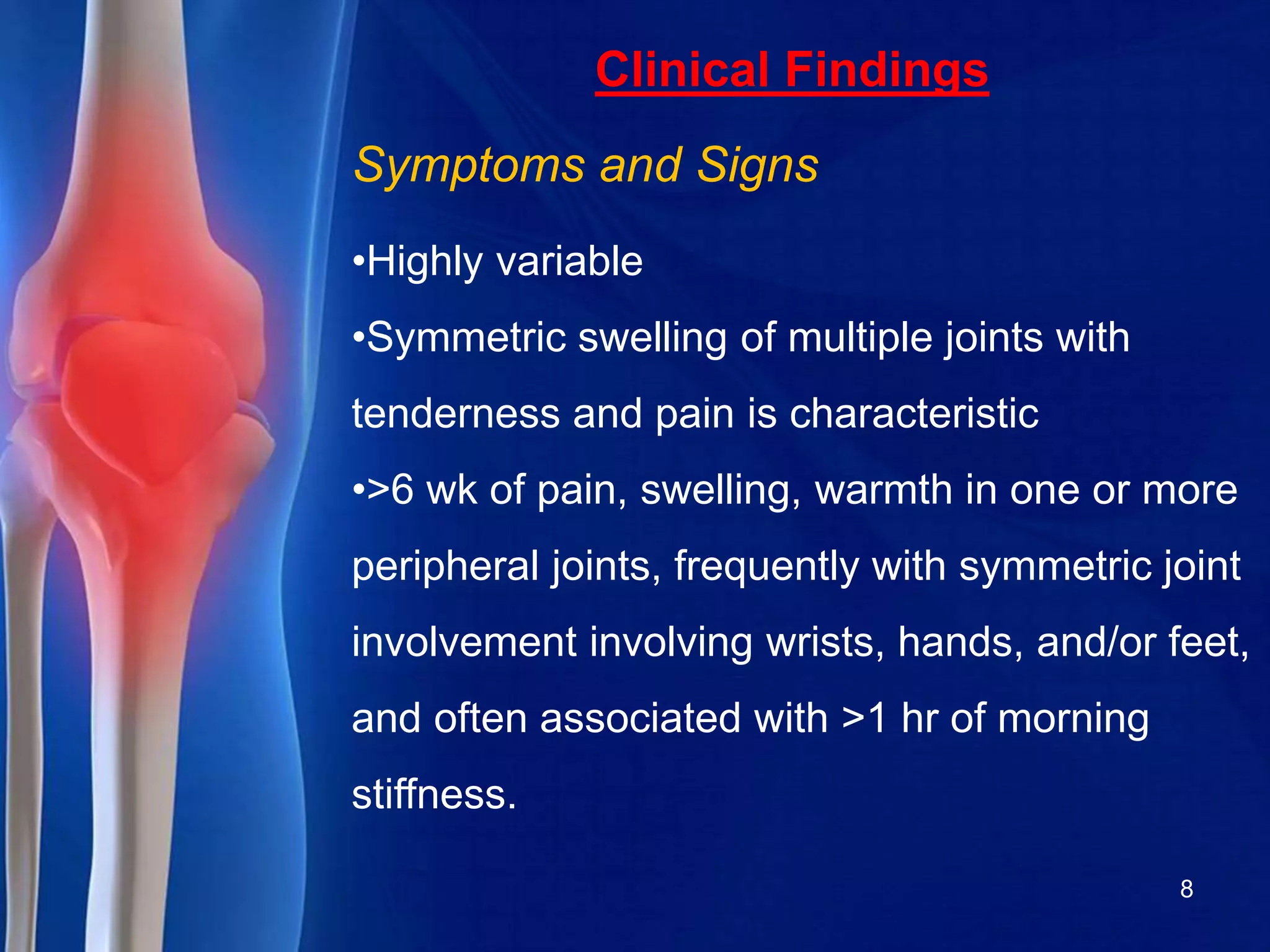
1. Morning stiffness lasting at least 1 hour*
2. Swelling in three or more joints*
3. Swelling in hand joints*
4. Symmetric joint swelling*
5. Erosions or decalcification on x-ray of
hand
6. Rheumatoid nodules
7. Abnormal serum rheumatoid factor.
[*Must be present at least six weeks]
14](https://image.slidesharecdn.com/rheumatoid-arthritisashwini-s-160215103426/75/rheumatoid-arthritis-14-2048.jpg)