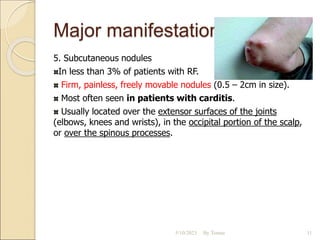
This document defines acute rheumatic fever as an indirect complication of group A streptococcal pharyngitis that primarily affects the heart, central nervous system, joints, and skin. It discusses the major manifestations of acute rheumatic fever such as carditis, migratory polyarthritis, Sydenham's chorea, erythema marginatum, and subcutaneous nodules. The modified Jones criteria for diagnosing acute rheumatic fever requires two major manifestations or one major and two minor manifestations along with evidence of a prior streptococcal infection. Treatment involves antibiotics, salicylates or steroids depending on symptoms, and long-term antibiotic prophylaxis to prevent recurrences.