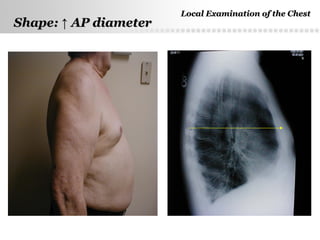
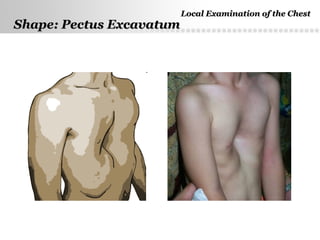
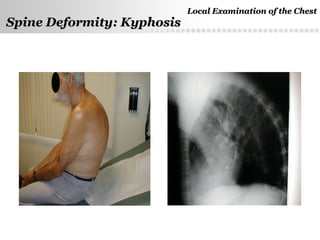
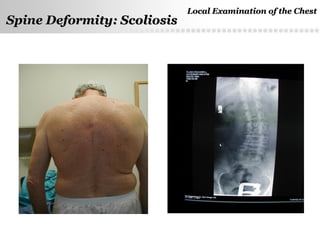
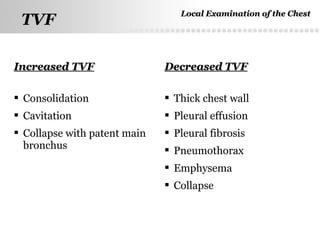
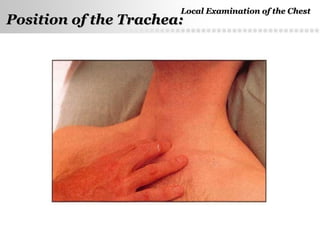
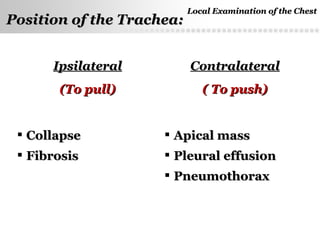
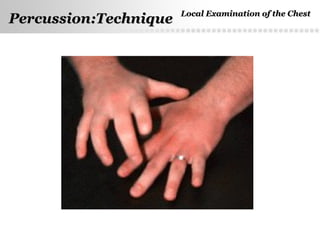
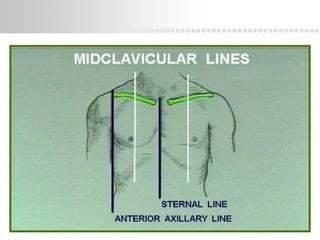
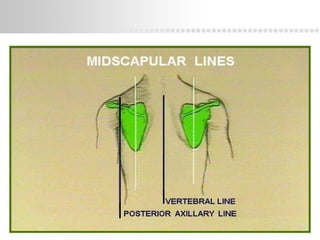
This document provides information on performing a local examination of the chest. It describes the key components of inspection, palpation, percussion, and auscultation. Inspection involves examining the shape of the chest and spine for any deformities. Palpation is used to confirm respiratory movements and feel for pulsations, adventitious sounds, and tracheal position. Percussion determines the lung borders and areas of dullness or resonance. Auscultation identifies breath sounds and adventitious sounds such as rhonchi or pleural rubs. Performing a thorough local chest exam provides important clinical information.













































![chapter 4 Physical diagnosis [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/physicaldiagnosisautosaved-250416123318-d2df54aa-thumbnail.jpg?width=640&height=640&fit=bounds)































