Download to read offline




















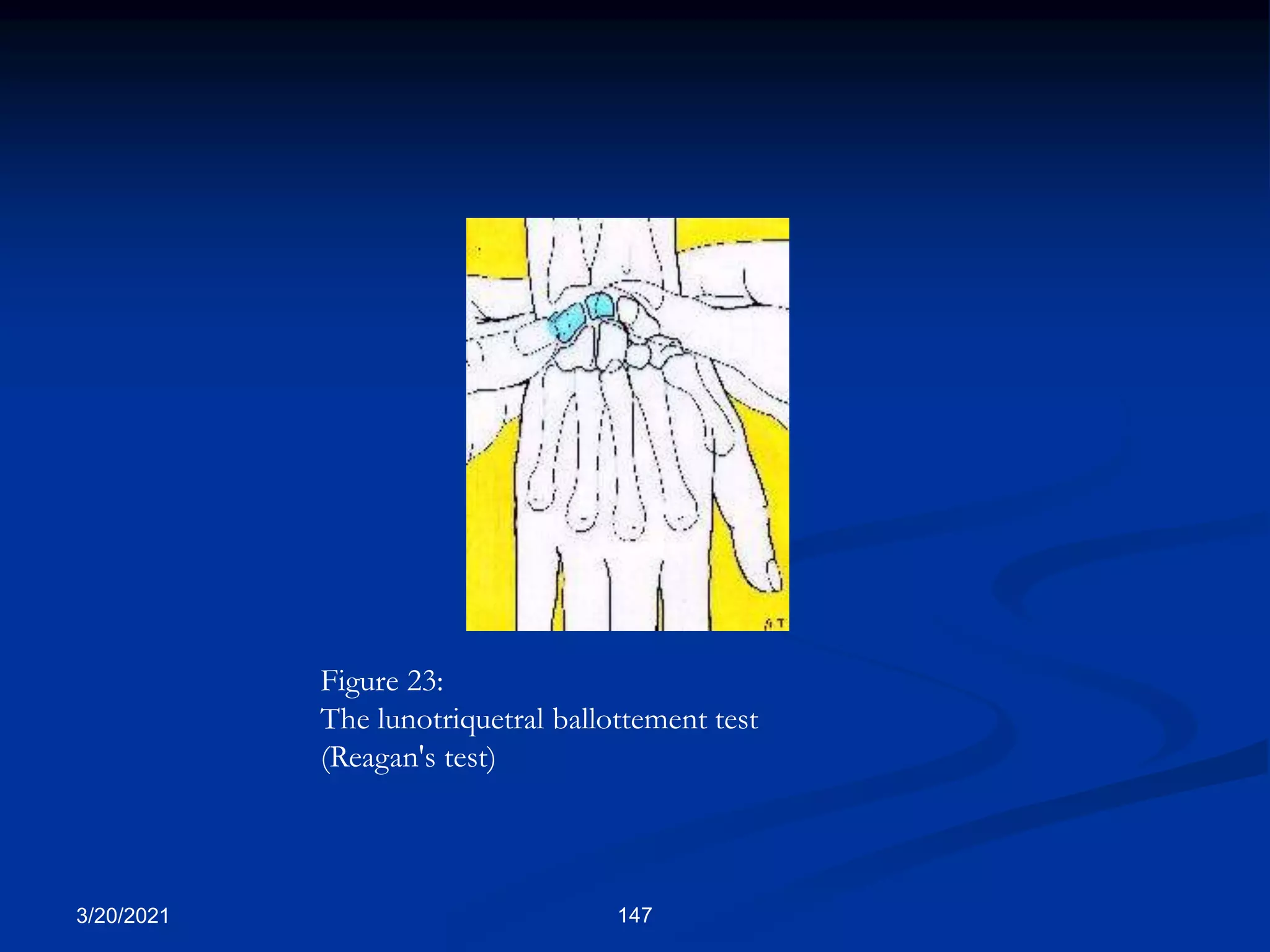
![The lunotriquetral ballottement test or Reagan's test (also called
the Shuck or shear test, depending on the authors):
as in the scapholunate ballottement test, the clinician holds the
lunate bone between his thumb and index finger with one hand,
and moves the triquetrum with the pisiform dorsal and palmar
(Figure 23). The aim is to appreciate instability (very difficult)
and above all the arousal of pain [30-32]. The sensitivity of this
test varies from 33 to 100%, depending on the authors, and its
specificity is still unknown.
3/20/2021 146](https://image.slidesharecdn.com/generalexaminationms2020-210320203629/75/General-examination-ms-2020-127-2048.jpg)
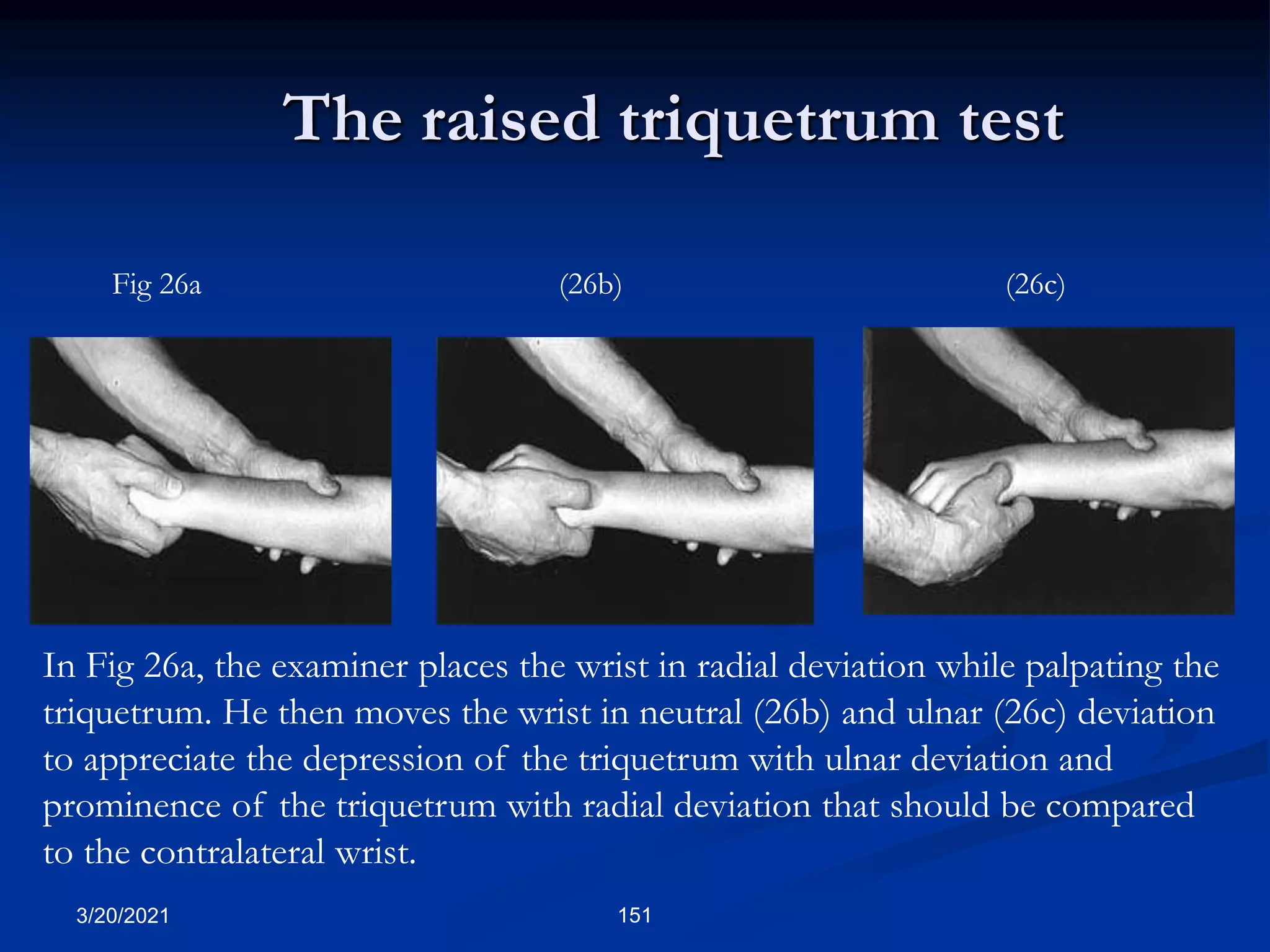
![The raised triquetrum test
was recently proposed by Zradkovic and Sennwald (personal communication).
The examiner holds the patient's hand proximal to the wrist and places his thumb on
the triquetrum.
From the neutral position, without flexion or extension, he performs radial and ulnar
deviation movements and appreciates the dorsal and palmar movements of the
triquetrum, which should be compared to those of the other wrist (Figures 26 a,b,c).
The sensitivity and specificity of this test are still unknown, as are the anatomical
lesions which cause the test to be positive.
As pointed out by Gilula, the triquetrum is very prominent or dorsal with radial
deviation, and moves palmarly and may even disapear with ulnar deviation.
On plain radiographs, the triquetrum is located "onto" or proximal on the hamate with
radial deviation (superposed), and "lateral" or ulnar to it with ulnar deviation
(juxtaposed) [Laredo, personal communication].
3/20/2021 150](https://image.slidesharecdn.com/generalexaminationms2020-210320203629/75/General-examination-ms-2020-131-2048.jpg)





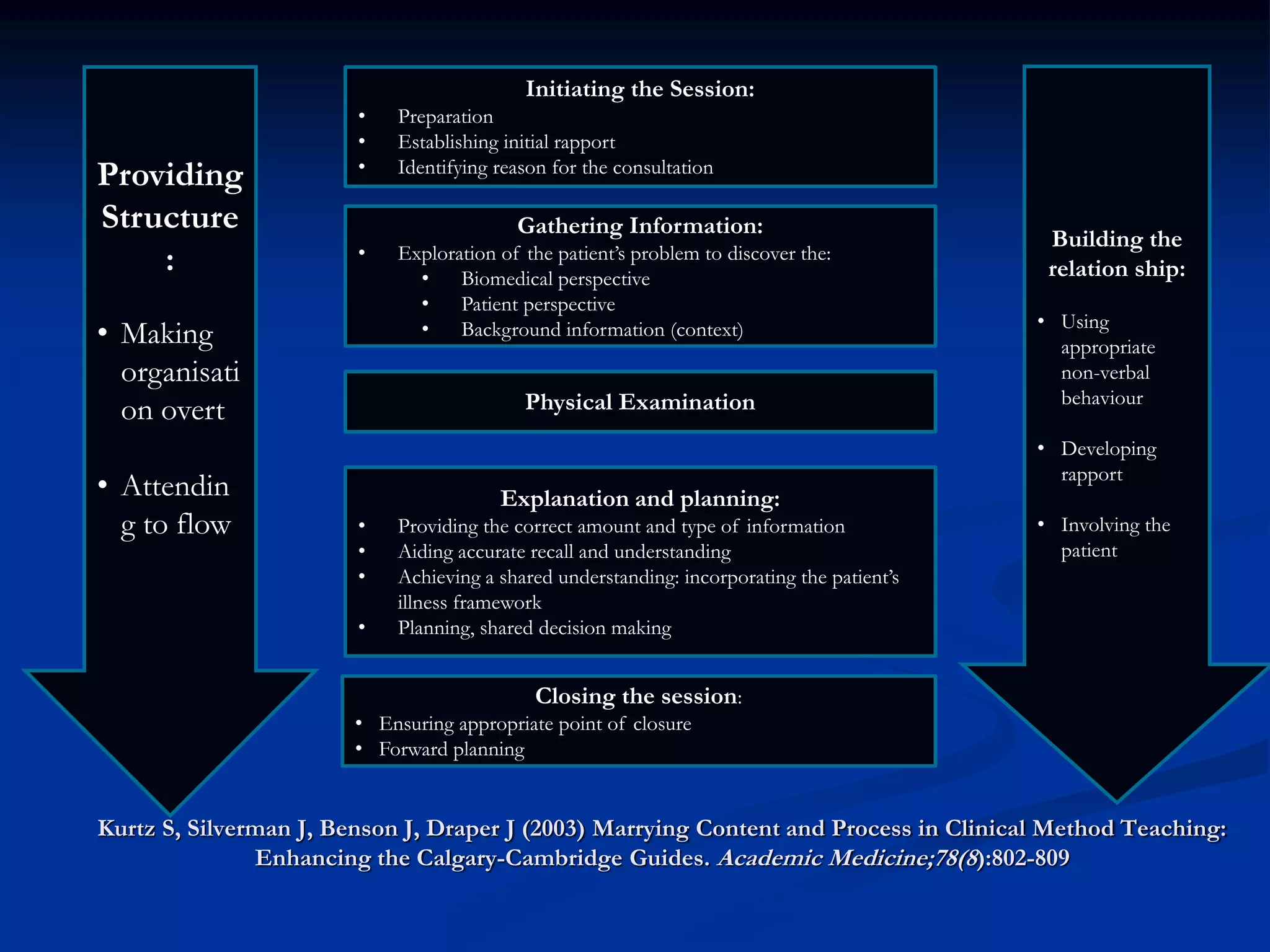
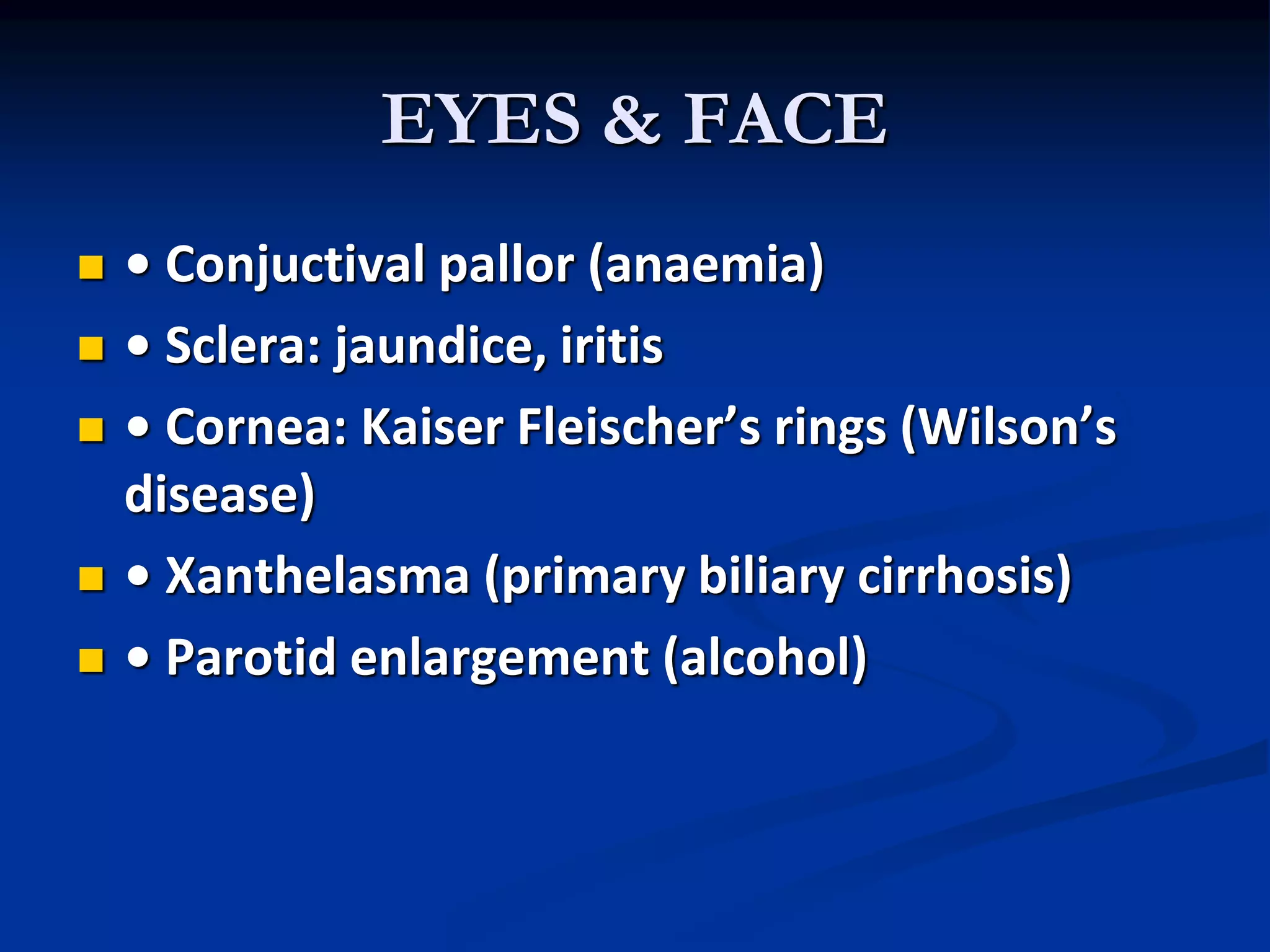
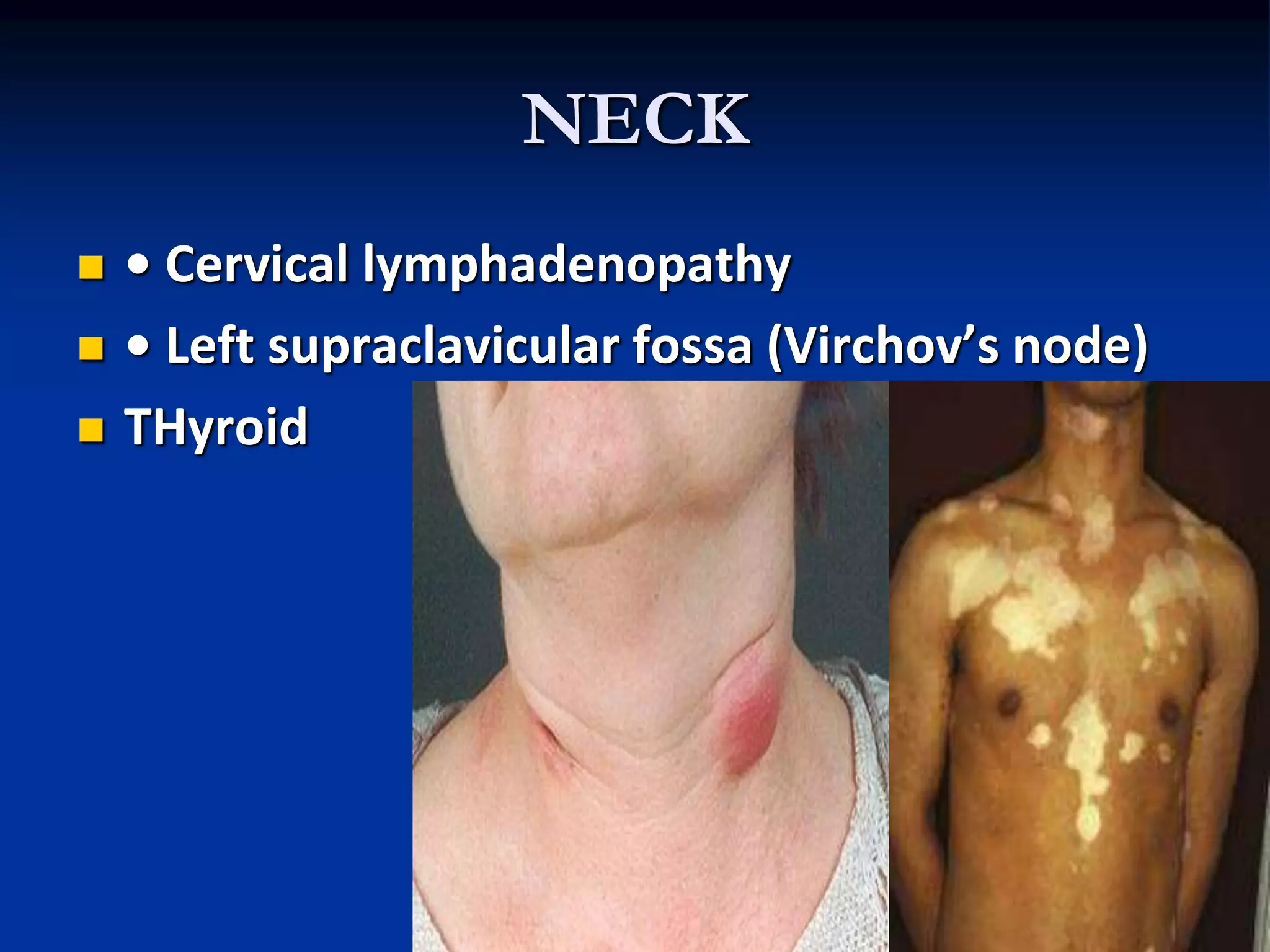
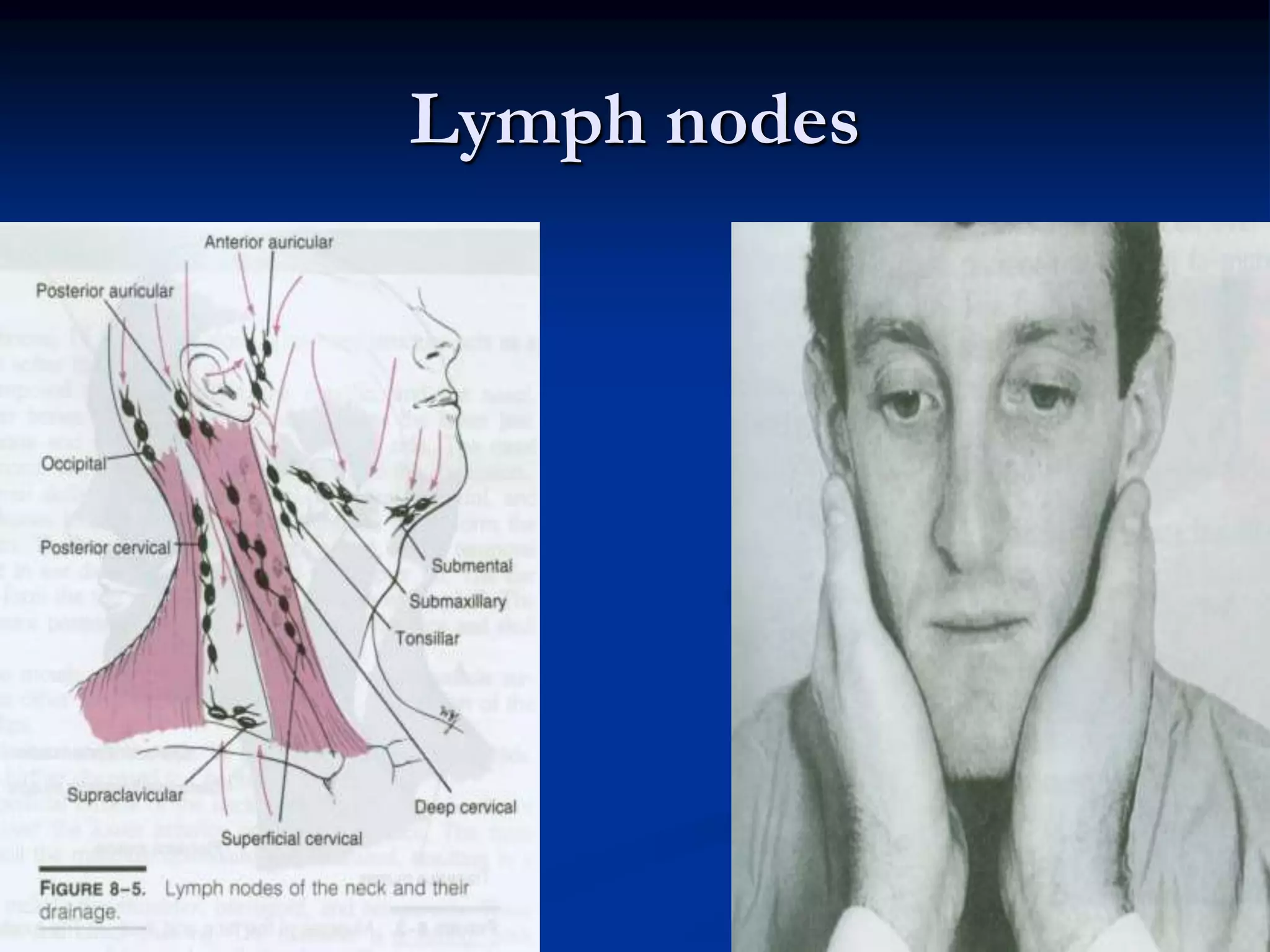
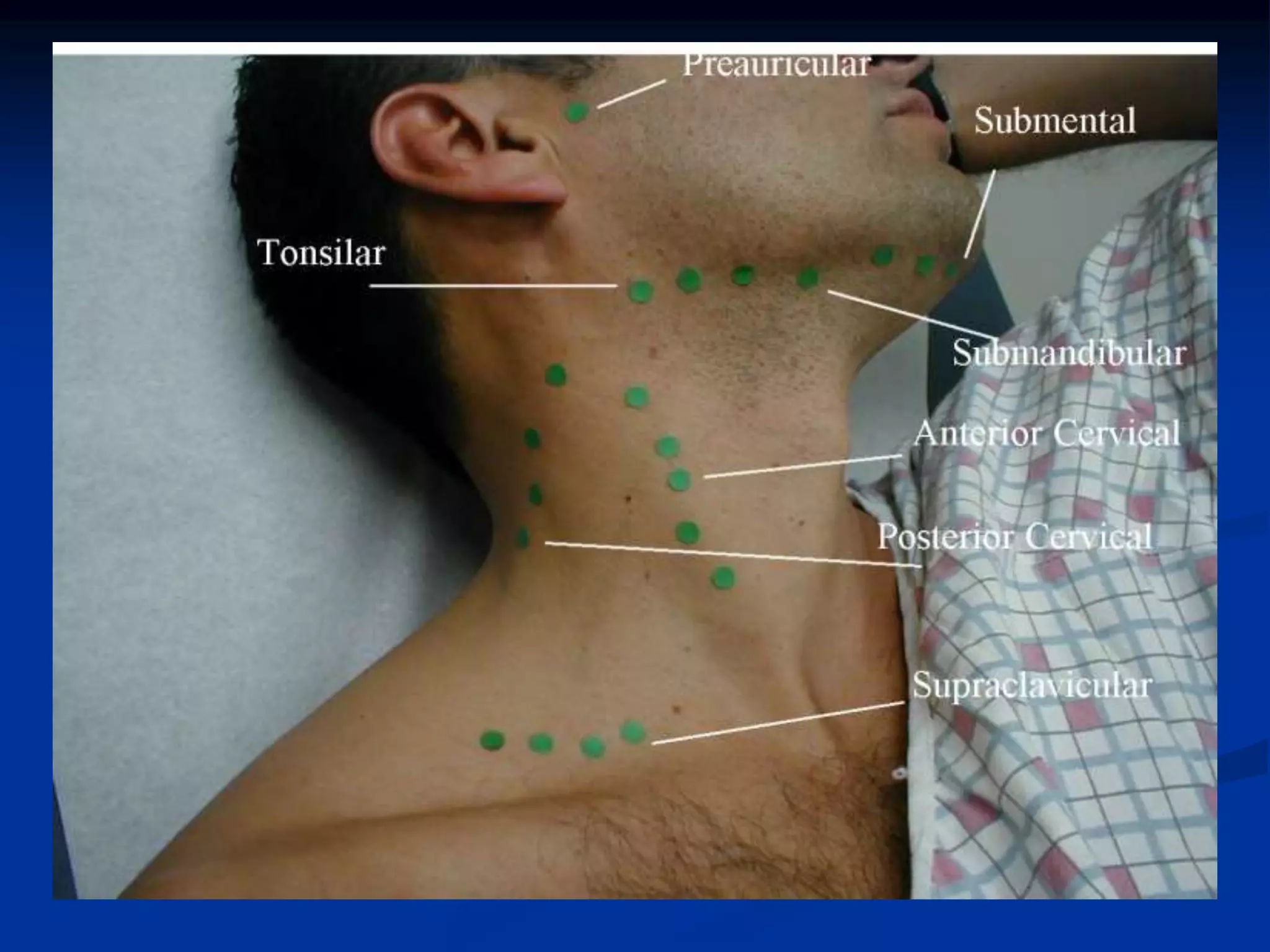
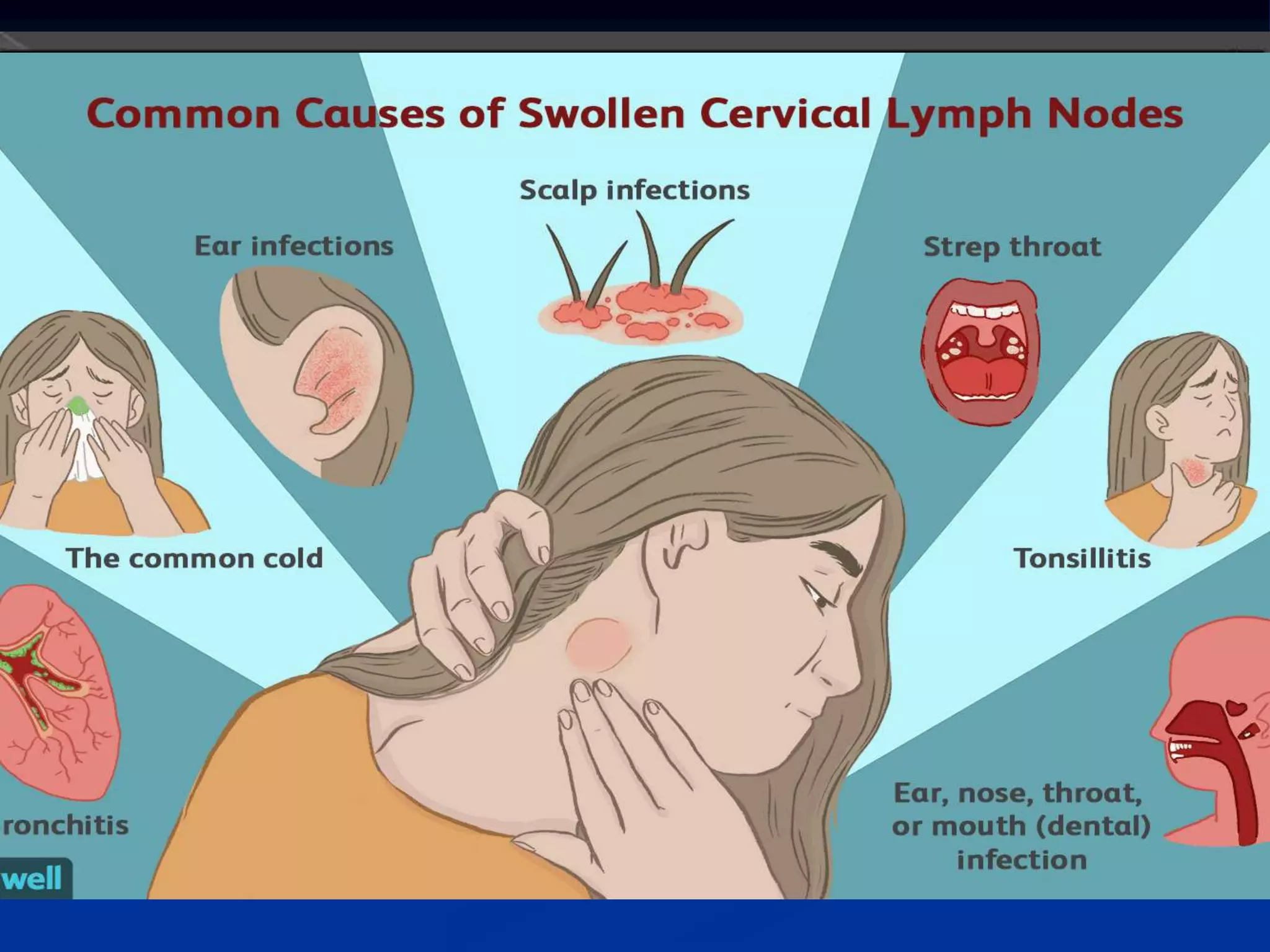
The document outlines best practices for clinical method teaching, emphasizing the integration of content and process in patient examinations. Key components include building rapport, effective history taking, and systematic physical examination techniques. It also details methods for assessing general health, specific conditions, and the importance of thorough inspection and documentation during patient interactions.


![Abdominal percussion [2015]](https://cdn.slidesharecdn.com/ss_thumbnails/abdominalpercussion2015-151117012348-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)


































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)

















