Glomerular disease postgraduate magdi sasi 2019
•
11 likes•657 views

RAMADAN KAREEM SMALL HINTS ABOUT GN FOR PSTGRADUATE DOCTORS

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Glomerular disease postgraduate magdi sasi 2019
Similar to Glomerular disease postgraduate magdi sasi 2019 (20)
More from cardilogy
More from cardilogy (20)
Recently uploaded
Recently uploaded (20)
Glomerular disease postgraduate magdi sasi 2019
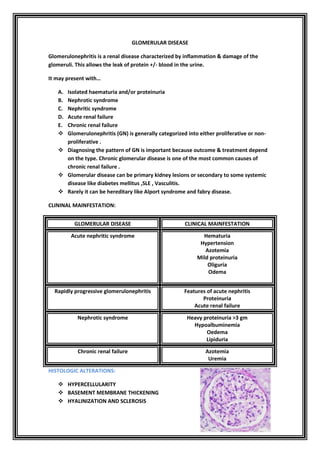
- 1. GLOMERULAR DISEASE Glomerulonephritis is a renal disease characterized by inflammation & damage of the glomeruli. This allows the leak of protein +/- blood in the urine. It may present with… A. Isolated haematuria and/or proteinuria B. Nephrotic syndrome C. Nephritic syndrome D. Acute renal failure E. Chronic renal failure Glomerulonephritis (GN) is generally categorized into either proliferative or non- proliferative . Diagnosing the pattern of GN is important because outcome & treatment depend on the type. Chronic glomerular disease is one of the most common causes of chronic renal failure . Glomerular disease can be primary kidney lesions or secondary to some systemic disease like diabetes mellitus ,SLE , Vasculitis. Rarely it can be hereditary like Alport syndrome and fabry disease. CLININAL MAINFESTATION: GLOMERULAR DISEASE CLINICAL MAINFESTATION Acute nephritic syndrome Hematuria Hypertension Azotemia Mild proteinuria Oliguria Odema Rapidly progressive glomerulonephritis Features of acute nephritis Proteinuria Acute renal failure Nephrotic syndrome Heavy proteinuria >3 gm Hypoalbuminemia Oedema Lipiduria Chronic renal failure Azotemia Uremia HISTOLOGIC ALTERATIONS: HYPERCELLULARITY BASEMENT MEMBRANE THICKENING HYALINIZATION AND SCLEROSIS
- 2. HISTOLOGIC CHANGES IN GLOMERULI CAN BE : 1. DIFFUSE:--involving all glomeruli 2. FOCAL:-- involving a few glomeruli 3. GLOBAL:--involving the entire glomerulus 4. SEGMENTAL:-- involving a apart of the glomerulus 5. MESENGIAL :--affecting predominantly the mesengial region. Non-Proliferative Glomerulonephritis: Characterised by the lack of proliferation of cells in the glomeruli Generally cause Nephrotic Syndrome Proliferative Glomerulonephritis Characterised by ↑ numbers of cells in glomeruli Usually presents with Nephritic Syndrome Dangerous! – can progress to end-stage-renal-failure over weeks to years
- 3. PATHOGENSIS OF GLOMERULAR INJURY: Immune mechanisms are responsible for most of the primary & secondary glomerular disorders. IMMUNE MECHANISMS OF GLOMERULAR INJURY 1. Antibody mediated injury: a. INSITU IMMUNE COMPLEX DEPOSITION Fixed tissue antigens present in kidney---- 1.Type IV collagen of the basement membrane 2. Heymann antigen ( basal surface of visceral epithelial cells ) 3. Mesangial antigens 4. Others b. PLANTED ANTIGENS: i. 1.Exogenous ( bacteria , drugs ) ii. Endogenous ( DNA , nuclear proteins ,immune complexes immunoglobulin 2. Circulating immune complex deposition A. Endogenous antigens ---DNA ,tumor antigens B. Exogenous antigens ----infectious products 3. Cytotoxic antibodies 4. Cell mediated immune injury 5. Activation of alternate complement pathway
- 4. RENAL SYNDROMES: 1) NEPHROTIC SYNDROME 2) NEPHRITIC SYNDROME 3) ACUTE RENAL FAILURE 4) CHRONIC RENAL FAILURE NEPHROTIC SYNDTOME N.S. is defined as the excretion of more than 3.5gm protein/24hours associated with hypoalbuminemia ,hypercholesterolmia and odema. MAINFESTATION OF N.S.: 1. MASSIVE PROTEINURIA 2. HYPOALBUMINEMIA 3. GENERALIZED OEDEMA 4. HYPERLIPEDEMIA AND LIPIDURIA Causes of nephritic syndrome: 1. PRIMARY GLOMERULAR DISEASE: DISEASE CHILDREN (( %)) ADULTS (( % )) MEMBRANOUS GLOMERULOPATHY 5 30 MINIMAL CHANGE DISEASE 65 10 FOCAL SEGMENTAL GLOMERULOSCLEROSIS 10 35 MEMBRANOGLOMERULONEPHRITIS 10 10 IGA NEPHROPATHY 10 15 2. SYSTEMIC DISEASES: A. Diabetes mellitus B. SLE C. Amyloidosis D. Drugs ----NSAIDS ,Heroin ,Penicillamine E. Infection ----malaria ,syphilis ,hepatitis B F. Malignancy ---carcinomas ,lymphoma G. Miscellaneous ---allergy , hereditary MINIMAL CHANGE DISEASE(( LIPOID NEPHROSIS )) Clinical : Most common cause of NS in children , 20—15% cases of NS in adults Selective proteinuria Sudden onset of sever NS , with hypoalbuminemia ,hypercholesterolemia ,normal BP/ GFR
- 5. Urinalysis ---4+ protein ,oval fat bodies ,hematuria in 20% cases Initial treatment ---steroids Does not cause progressive renal failure with good prognosis. Diagnosis is by renal biopsy. BIOPSY: Notice the four black arrows in the normal specimen. They are pointing out a normal feature of kidney cells called “foot processes”. These foot processes are an important part of the kidney filters themselves, and are essential for determining what gets filtered out of and what stays in the circulation. The individual foot processes can no longer be made out- it is like they have all just “melted” together into a single thin layer. This important barrier in the filtration process can no longer keep protein from being filtered out of the blood and into the urine. L.M. finding : no glomerular abnormality I.F .finding : no glomerular Ig deposits (( occasionally Ig M)) E.M. finding : diffuse foot process effacement
- 6. How did the patient get it? Minimal Change Disease is one of the most common causes of the Nephrotic Syndrome , especially in children. In fact, almost 90% of children 10year and under with the Nephrotic Syndrome end up having MCD when biopsied (as opposed to 20% of adults). It is of two categories, primary and secondary. Secondary means that the MCD was caused by, or is at least associated with, another medical condition. MCD has been associated with all of the following, usually in adults: 1. Drugs NSAIDs, lithium, some antibiotics, bisphophonates 2. Malignancy Leukemia, Lymphoma 3. Infection Syphillis, HIV, Hepatitis 4. Allergy Associated with multiple environmental allergies Secondary MCD is very uncommon, and a diagnosis of MCD does not need any a “workup” for any of the above conditions. What are the symptoms? The clinical presentation is Nephrotic Syndrome. This syndrome always includes- 1. >3 g proteinuria per day 2. Hypoalbuminemia 3. Generalized edema (swelling)` 4. Hyperlipidemia (high cholesterol) Hypercoagulability (increased tendency to form blood clots) The most noticeable symptom of MCD is often edema, or swelling, which can be profound. This typically starts in the feet and legs, but can move into the hips and abdomen as well. In contrast to many of the other diseases that can cause the Nephrotic Syndrome, the proteinura and edema of MCD can develop very rapidly- almost overnight. Unlike the majority of other kidney diseases, especially those that cause the Nephrotic Syndrome, the ability of the kidney to clean the blood is often unaffected in MCD. This is especially true in children and young adults. None of the above symptoms, or even all of them together, is specific for MCD. If your doctor are concerned about MCD, the only way to know for sure is to have a kidney biopsy. However, because of how common this disease is in children, when a child is diagnosed with the Nephrotic Syndrome he is typically treated for Minimal Change Disease before undergoing a biopsy. If this therapy does not immediately improve symptoms and decrease the amount of protein in his urine, then a biopsy to look for another cause is considered. What is the treatment? Minimal Change Disease is one of the more treatable kidney diseases, especially in children. Therapy almost always consists of a course of oral steroids (prednisone), which is generally effective within weeks. A complete remission is not uncommon, though the disease can come back later in life. Patients with recurrent MCD, or with MCD that does not completely resolve with steroids, may require other forms of chemotherapy.
- 7. It is also important for someone with MCD to be on medication that reduces the amount of protein in the urine. These are ACE-inhibitors (angiotensin converting enzyme inhibitors) and ARBs (angiotensin II receptor blockers). If urine protein levels are high, the complications of the Nephrotic Syndrome should also be considered; patients should receive routine cholesterol screening/treatment, and remember their tendency to form clots(( anticoagulant)) . FOLLOW UP: Every patient with MCD must have their kidney function monitored regularly. If kidney function declines, certain other interventions may become necessary. What is the prognosis? Even in adults, Minimal Change Disease typically has a favorable prognosis. Over 90% of patients will respond to oral steroids, with most of these having a complete remission. However, more than 50% of the adults who go into remission will relapse at some point in their lives, and for these patients either another course of steroids or another form of chemotherapy entirely may be necessary. Although it is rare for Minimal Change Disease itself to lead to End Stage Kidney Disease, some patients with MCD eventually develop another disease called Focal Segmental Glomerulosclerosis (FSGS). FSGS is generally seen as a more aggressive disease, with less treatment options and more of a tendency towards eventual kidney failure. SUMMARY: MCD ---present with nephrotic syndrome Common in children Can be 1ry or 2ry to drugs ,infections , CTD Generalized edema within 24 hours is characteristic Respond to steroids High risk of DVT ,renal artery thrombosis Need heparin while the patient is under treatment in hospital Diagnosed by 24 hour urine collection for proteinuria , decreased serum albumin with Hypercholestremia in blood with edema as the only clinical sign
- 8. MEMBRANOUS GLOMERULOPATHY: Clinical : Non selective type of proteinuria Most common cause of nephrotic syndrome in adults ,after FSGS. Most frequently is idiopathic . It can be associated with chronic antigenic stimulation : infections (( HBV , HCV ,Syphilis ,Malaria )) , cancer , mediaction (( gold ,penicillamine )) systemic diseases(( thyroditis ,SLE )). 50% of cases have hematuria Prognosis is variable . Although mild cases have spontaneous remission ,some patients evolve to ESRD. Diagnosis is confirmed by renal biopsy. What is Membranous Nephropathy? Membranous Nephropathy (MN) is a kidney disease that can occur by itself (primary) or in conjunction with several other diseases (secondary). MN is one of the most common causes of the nephrotic syndrome in adults. Over time this can lead to kidney failure as well. MN is caused by the build- up of immune complexes within the kidney itself. Immune complexes are made when a person’s antibodies attack something they consider foreign to the body (an antigen). This is often an infection of some sort. An antibody +an antigen = an immune complex. These immune complexes are normally eliminated while still in the circulation. BIOPSY: L.M. finding: normal glomeruli or thick glomerular capillary basement membrane ,normal cellularity , spikes on silver stains. I.F.findings: Granular IgG and complement are present along glomerular capillary loops. E.M. findings: subepithelial electron –dense deposits and foot process effacement. PATHOGENSIS: An insitu I.C. formation and complement activation . Ag in experimental models is Gp 330 (( Heyman Ag )) in coated pits of epithelial cells .Ag can also be entrapped or planted.
- 9. The antibodies floating in the blood pass through the vessel wall and encounter the antigen. The resulting immune complexes become stuck in that space. Over time they begin to further activate the immune system. This activation causes inflammation and damages the kidney itself. This damage can be seen under the microscope as a “thickening” of the vessel walls within the kidney filters. How did I get it? MN usually occurs in adults older than forty, and is fairly rare in children. Men are affected more often than women. Whites are affected more commonly than blacks. Though we know how the kidney damage occurs in MN, we don’t know exactly why the immune complexes occur in all people. In these cases the disease is called Primary MN.
- 10. In Secondary MN, the same type of kidney injury occurs but is associated : a) Systemic Lupus Erythematosis (Lupus) b) Hepatitis B and C c) Cancers (especially of the lung or colon) d) Drugs, such as penicillamine, gold, and non-steroidal anti-inflammatory drugs. Anyone who is found to have MN, especially those over 50 years old, should be tested for Hepatitis and undergo routine age-appropriate cancer screening. SYMPTOMS: MN often causes the Nephrotic Syndrome . The most noticeable symptom of MN is often edema, or swelling, which can be serious. This typically starts in the feet and legs. But it can move into the hips and abdomen as well. Other symptoms include high blood pressure, high cholesterol, and a tendency to form blood clots. Protein levels can be measured in a urine sample. Kidney function can be calculated from a blood test alone or measured more directly using a 24-hour urine collection. MN can cause protein in the urine alone. It can also cause protein in the urine and kidney failure together. None of the above symptoms or even all of them together, is specific for MCD. If the doctor are concerned about MN, the only way to know for sure is to have a kidney biopsy. What is the treatment? MN is not an easy disease to treat. 1. Should be seen regularly by a kidney specialist. 2. It is important to be on a medication that reduces the amount of protein in the urine. ACE-inhibitors and ARBs 3. If urine protein levels are high, the complications of the Nephrotic Syndrome should also be considered—anticoagulant to avoid DVT ,PE. 4. Patients should receive routine cholesterol screening/treatment. 5. Finally, patients with MN must have their kidney function monitored regularly. If kidney function declines, certain other interventions may become necessary. 6. Immunosuppressants are also being used to treat MN. The most common of these are steroids. For MN this is often combined with another type of chemotherapy, such as cyclophosphamide or chlorambucil. Unfortunately, all of these drugs have significant side effects. Their use must be considered on a patient-by-patient basis. In secondary MN , it is most important to treat the underlying disease (infection, cancer, or autoimmune) or to stop the causative drug. Often this is enough to get rid of, or at least significantly improve, the kidney disease. What are the chances of getting better? Up to 40% of patients with MN undergo a spontaneous remission within 5 years, even without therapy. These patients do not necessarily stay in remission, however. On average, 20 years after diagnosis, 1/3 complete remission, and 1/3 progressed to end- stage renal disease and need dialysis. Another 1/3 will be somewhere in the middle. Those people that initially have more than a gram of protein in their urine per day for more than six months tend to do worse. Their renal function often declines regardless of therapy. Kidney Transplant in Membranous Nephropathy: Unfortunately, many patients diagnosed with MN will eventually progress to kidney failure. Fortunately, kidney transplant is a treatment option for these patients.
- 11. FOCAL SEGMENTAL GLOMERULOSCLEROSIS It is a relatively common form of kidney disease, especially in the US. Although there are several known risk factors, we don’t yet know why most people develop FSGS. FSGS is named for the scarring, or “sclerosis,” ((found in the kidney of people)). When glomeruli are damaged they become scarred. They are no longer able to filter blood appropriately. This is called “glomerulosclerosis”. The word “focal” is added because in FSGS, only some of the filters are damaged. “Segmental” is included because often only parts of the filters are scarred. Clinical : Most common cause of idiopathic NS in adults ,especially African-Americans. The disease is twice as common in blacks than in whites. Occurs in all age groups ,very heterogenous disease . HTN and reduction in GRF common. Non selective proteinuria. When nephritoc syndrome does not respond to treatment ,the prognosis is poor . It may evolve to ESRD . Most common cause of nephritic syndrome and renal failure associated with HIV infection. How is at risk? No one is sure. There are two big categories, primary and secondary. These are some of the secondary causes/associations. a) Kidney defects from birth b) Urine backing up into kidneys-- Reflux nephropathy c) Viruses –HIV 1 ,parvovirusB19 ,CMV ,EBV, simian virus 40 d) Heroin ,Interferon α β Ɣ ,lithium , lithium ,pamidronate ,sirolimus anabolic steroids ,calcineurine inhibit nephrotoxicity e) Adaptive –mediated by adaptive structural and functional response to glomerular HTN caused by elevated glomerular capillary pressure and flow: Conditions with reduced renal mass---oligomeganephronosis ,very low birth weight , renal dysplasia ,cortical necrosis causes ,reflux nephropathy ,renal allograft ,aging kidney ,surgical renal ablation f) Conditions with normal renal amss—HTN ,acute or chronic veno-occlusive processes (( atheroembolization ,thrombotic microangiopathy ,renal artery
- 12. stenosis)) ,increased body mass index (( obesity ,body building –increased lean body mass )) ,cyanotic congenital heart disease, Sickle Cell Anemia g) Obstructive Sleep Apnea Secondary focal segmental glomerulosclerosis from exposure may be due to virus-induced or drug-induced disease. Viruses can act on the podocyte either by direct infection or by the release of inflammatory cytokines that interact with podocyte receptors. The best studied of such viruses is human immunodeficiency virus type 1 (HIV-1), which directly infects podocytes and tubular epithelial cells. The form of focal segmental glomerulosclerosis associated with untreated HIV-1, called HIV-associated nephropathy (HIVAN), typically progresses rapidly and is associated with glomerular collapse. Parvovirus B19 is another virus that can infect podocytes and tubular cells, leading to collapsing focal segmental glomerulosclerosis. Other viruses associated with this disease, such as simian virus 40, cytomegalovirus, and Epstein-Barr virus, are less well characterized. Heroin use is associated with focal segmental glomerulosclerosis, though the incidence of this drug-induced disease has fallen sharply in parallel with the increasing purity of modern street heroin. The bisphosphonate pamidronate, an osteoclast inhibitor, has been linked to the development of focal segmental glomerulosclerosis. All forms of interferon therapy, including interferon-alfa (widely used to treat hepatitis C), interferon-beta (indicated for multiple sclerosis), and interferon-gamma have been reported to induce focal segmental glomerulosclerosis. In the transplanted kidney, toxic effects from calcineurin inhibitors as well as sirolimus are associated with development of focal segmental glomerulosclerosis Most people with the above conditions do not have FSGS. Having FSGS does NOT put patient at risk for any of these conditions if he do not already have. However, having family members with FSGS does increase the patient chances of developing it yourself. Also, the disease is twice as common in blacks than in whites. What are the symptoms? Proteinuria is a defining feature of Fssg .GS can cause nephrotic syndrome. Many people with FSGS have no symptoms at all. The most common complaint is edema, or swelling, especially in the legs. Often patients find that their shoes no longer fit, or that they have suddenly put on weight. High blood pressure, or hypertension, is also a very common finding. The hypertension in people with FSGS can often be very difficult to treat. A blood test, urine tests, and a kidney biopsy will determine glomerulosclerosis. FSGS can also cause abnormal results in two different routine laboratory tests . The first is renal function test kidney (( urea and “creatinine")) .A higher level of creatinine is expected finding .
- 13. The second test is for protein in your urine. Some people with a large amount of protein in their urine say that their urine looks “foamy,” like bubbles built up in dishwater. Biopsy: Having a low GFR and protein in the urine is not proof of glomerulosclerosis, though. Since these are associated with other kidney conditions, a kidney biopsy is needed to diagnose glomerulosclerosis. The diagnosis is made from the signs of scarring seen on the kidney tissue sample. Treatment :----- usually steroids and ACE-I Diagnosis is confirmed by renal biopsy. BIOPSY: L.M.findings---- focal segmental glomerular sclerosis I.F. findings --- IgM deposition in the mesangium in some cases. E.M. findings ---- severe foot process effacement ; in patients with AIDS , INTRACYTOPLASMIC TUBULORETICULAR structures and test tubes are observed by EM. PATHOGENSIS: Probably glomerular hyperfiltration . Exact mechanism unknown. Which clinical and pathologic features predict outcome FSSG? A: Black race, increased degrees of proteinuria and renal insufficiency, and severity of interstitial fibrosis and tubular atrophy in biopsy specimens are associated with a worse outcome. Patients with a partial or complete remission of proteinuria have better outcomes than those who do not. The prognosis in the hemodynamic adaptive form of the disease is typically much better than in the primary, possibly as a consequence of an increased likelihood of complete or partial remission with RAS inhibition in this
- 14. population In the tip variant, the glomerular scarring and damage occurs at the “tip” of the filter. This “tip” is the beginning of the tube that carries away the urine, and it is usually on the opposite side of the filter from where the blood vessels enter and exit. In the picture on the left, the tip is at the top- you can see that the green tube exiting the top of the filter is blocked with a scar. The symptoms of FSGS in the tip variant often appear suddenly. There is a large amount of protein in the urine and a tendency to develop the full Nephrotic Syndrome .This variant also seems to be the most responsive to treatment, with most of the patients who receive steroids undergoing a full or partial remission. The perihilar variant has scar that forms at the hilum of the filter. This is where the blood vessels enter and exit. The hilum is at the bottom of the filter. In this variant, the cause of the FSGS is often something that has previously caused a reduction in the number of filters someone has. Being born with only one kidney or having significant kidney damage early in life from reflux nephropathy can cause this type of damage.
- 15. The collapsing variant is considered the most rapidly progressive form of FSGS. It does not typically respond to therapy. The scarring quickly affects the entire filter, causing it to collapse. Most patients that are diagnosed with the Collapsing variant will require dialysis or a kidney transplant within one to two years despite treatment. This variant was previously thought only to effect people with HIV. It is now found in increasing numbers of HIV-negative patients. Collapsing FSGShas also been associated certain drugs, such as pamidronate. The cellular variant implies a slightly different type of scarring. The problem is an overabundance of cells that make up the filter itself. As these cells build up, the blood vessels that make up the filter narrow and eventually close off completely. This variant can only be diagnosed if none of the above variants are seen on the biopsy. Classic FSGS If none of the above specific variations are seen on biopsy, the disease is called Classic FSGS, or FSGS NOS. This stands for “not otherwise specified”. This form is generally less severe than the collapsing form. But having a diagnosis of Classic FSGS does not indicate how severe the disease will be, or how it will respond to treatment.
- 16. FSGS is not an easy disease to treat. Once a diagnosis is established on biopsy, potential secondary causes that require specific therapies should be ruled out before a patient is presumed to have primary focal segmental glomerulosclerosis. For example ; The form of the disease that is caused by HIV-1 ----- antiretroviral therapy Drug-induced forms are managed by discontinuation of the inciting agent. 1. Dietary sodium restriction as initial therapy. 2. It is also important for someone with either primary OR secondary FSGS to be on medication that reduces the amount of protein in the urine((ACE-inhibitors and ARBs)). 3. Many immunosuppressant are used to treat FSGS. The most common of these are steroids . Glucocorticoid and calcineurin inhibitor therapies are successful in approximately 50% of patients... Unfortunately, all of these drugs have significant side effects. Their use must be considered on a patient-by-patient basis. 4. Other therapies have been tried, including alkylating agents, plasmapheresis, and even the anti-B-cell monoclonal antibody rituximab, which also stabilizes the podocyte actin cytoskeleton, but none of these therapies have been shown to be effective 5. If urine protein levels are high, the complications of the Nephrotic Syndrome should also be considered. Patients should receive routine cholesterol screening/treatment. Every patient with FSGS should have their RFT monitored regularly with both blood and urine studies. COURSE? If not treated, most patients with FSGS will eventually develop complete renal failure and require dialysis or a kidney transplant to survive. Even with treatment, many patients will still eventually require dialysis. How long this will take varies widely (2-20 years), and is difficult to predict. Specific forms of FSGS have been associated with different rates of progression and responsiveness to therapy. Kidney Transplant in FSGS: Unfortunately, many patients diagnosed with FSGS will eventually progress to kidney failure. Kidney transplant is a treatment option for these patients. The risk of FSGS returning in the transplanted kidney varies from 20-50%. The risk factors that put patients at higher risk of recurrence of FSGS are: 1. Young age (< 15 years old) 2. If it took less than 3 years from the time the FSGS was found in original kidneys to reach kidney failure 3. The appearance of certain cells on original kidney biopsy. 4. Caucasian (White) race 5. If the patient lost a previous kidney transplant to a return of FSGS Usually a return of FSGS in the transplant occurs very soon after the surgery. The FSGS can return within hours to days. Most episodes will be within the first year after transplant.
- 17. Over half of the patients with recurrent FSGS in their transplant will lose their kidney within 5 years. Of all the patients with FSGS who get a kidney transplant, about 15% will lose the kidney due to recurrent FSGS.
- 18. FSSG Primary FSSG with FSSG with nephritic Adaptive 2ry drug ,virus Subnephrotic proteinuria RAS inhibition and Na restriction RAS inhibition and Na restriction TR cause Glucocorticoid daily or alternative + RAS inhibition No response/worsening disease OR C.I. IF STEROID INTOLERANCE Adult 16 weeks ,children 4-6 weeks treatment GLUCOCORTICOID RESISTANT CALCINEURINE INHIBITION
- 19. NEPHRITIC SYNDROME((POSTSTREPTOCOCCAL GN)) Clinical Nephritic syndrome usually follows a 6 –14 day latent period after a group A beta –hemolytic streptococcal infection or a longer latent period after skin infection. Treatment of infections has decreased incidence of postinfectious GN. Usually presents as –gross hematuria ,edema and hypertension. Reduce C3 and C4 during first 6 – 8 weeks. Identical clinical picture can be with complete recovery of renal function particularly in children. Biopsy is performed only in cases with atypical presentation. This condition can occur at any age. However, it is mostly common in children ages six to ten. This condition is also known to affect twice as many males than females. Biopsy L.M. findings ---hypercellular glomeruli are observed I.F. findings ---deposition of IgG and of complement ,with a granular pattern ,along glomerular capillary loops. E.M. findings----confirms the presence of subepithelial electron dense deposits. In some cases, it is possible to see well-defined rounded deposits outside of the capillary walls which look like humps. The presence of these humps may be a sign of Post-Infectious GN. But it can also be seen in other types of glomerulonephritis.
- 20. How did the patient get it? The immune system protects us against diseases by finding and killing bacteria. Bacteria and its toxins, which are called antigens, activate the immune system. The immune system then builds antibodies which bind to the toxin. This binding activates another part of the immune system which is called the complement system. This system is responsible for destroying these bacteria. In other words, antibodies find the target and complement destroys it. In the case of Post-Infectious GN, these immune complexes (formed from antigen, antibodies, and complement) get trapped in the kidney filters. The filters become inflamed, which leads to ineffective kidney function. Not everybody who has a sore throat or skin infection develops this type of glomerulonephritis. For this reason it is thought that there are some genetic factors that put people at risk for this. Pathogenesis : In situ I.C.formation and complement activation. The Ag is possibly a planted cationic bacterial protein. What are the symptoms? The symptoms of this condition are fluid retention with generalized swelling; swelling of the abdomen; swelling of the face or eyes; swelling of the feet, ankles, and arms and legs. Symptoms also include high blood pressure, Coca-Cola colored urine, blood in the urine, decreased amount of urine, joint stiffness and joint pain How is Post-Infectious Glomerulonephritis diagnosed? Blood pressure is often high Physical examination shows swelling, especially of the face Blood testing shows indicators of a specific type of recent infection.
- 21. Serum complement levels are usually decreased Urinalysis shows protein and blood in the urine Kidney biopsy confirms Post-Infectious GN, although biopsy is not usually necessary What is the treatment? There is no specific treatment for Post-Infectious GN. Treatment is focused on relieving symptoms. Antibiotics, such as penicillin, should be used to treat any bacterial infection. Blood pressure medications and diuretic medications may be needed to control swelling and high blood pressure. Dietary salt restriction may be necessary to control swelling and high blood pressure RAPIDLY PROGRESSIVE GLOMERULONEPHRITIS (( CRESENTRIC GN )) 1. TYPE I RPGN ( ANTI-GBM ANTIBODY ) Idiopathic Good pasture syndrome 2. TYPE II RPGN ( IMMUNE COMPLEX ) Idiopathic Post infectious SLE Henoch –Schonlein purpura Others 3. TYPE III RPGN ( PAUCI IMMUNE ) ANCA associated Idiopathic Wegener granulomatosis Polyarteritis nodosa /Microscopic polyangitis MEMBRANOPROLIFERATIVE GN Membranoproliferative glomerulonephritis (MPGN) is a disease that affects the glomeruli, or filters, of the kidneys. Most instances of MPGN are caused by other diseases or disorders, including autoimmune diseases (such as systemic lupus erythematosis), chronic infections (like hepatitis B or more commonly hepatitis C), monoclonal immunoglobulin deposition diseases, and hereditary diseases. However, a few cases are idiopathic, or of unknown cause. The idiopathic type of MPGN is seen more commonly in persons aged 8-30. Who is at risk? As stated above, MPGN is usually found in patients who have other diseases. The diseases associated most often are: 1. Autoimmune diseases (most often systemic lupus erythematosus) 2. Hepatitis B infection 3. Hepatitis C infection 4. Cryoglobulinemia 5. Monoclonal immunoglobulin deposition diseases (such as AL amyloidosis and light and heavy chain deposition diseases) 6. Subacute bacterial endocarditis 7. Infection of a ventriculoatrial shunt 8. Chronic lymphocytic leukemia (CLL)
- 22. So, if a patient is diagnosed with MPGN, the above associated diseases should be tested for and ruled out before the MPGN is considered idiopathic (of unknown cause). Also, as noted above, the idiopathic type of MPGN is seen more commonly in persons aged 8-30. What are the symptoms? The symptoms of MPGN are very similar to those of a focal glomerulonephritis. Specifically, patients have hematuria (blood in the urine), either macroscopic, which can be seen by the naked eye, or microscopic. Many of the red blood cells are dysmorphic (malformed or misshapen). In addition, mild or severe proteinuria can be found (including the nephrotic syndrome). MPGN TYPE I---MESANGIOCAPILLARY GN Type I – Discrete immune complexes are found in the mesangium and subendothelial space. This activates the immune system, which causes inflammation and damage to the kidney itself. Clinical Can present as an acute nephritic syndrome with nephrotic syndrome. Frequently associated with hepatitis C virus More common in adolescents and children Complement activation occurs in only 50% of cases in adults Not a frequent disease Diagnosis by renal biopsy Biopsy L.M. finding--- hypercellular lobulated glomeruli with double capillary basement membrane on special stains. I.F.findings ---demostrates IgG ,IgM and complement at the periphery of the glomerular lobules E.M. findings--- subendothelial electron dense deposits and new basement membrane deposition are observed . Pathogenesis: Deposition of circulating IC complement activation
- 23. Type II – This is also called dense deposit disease. When viewed under the microscope, continuous, dense ribbon-like deposits are found along the basement membranes of the glomeruli, tubules, and Bowman’s capsule.
- 24. Type III – This is also an immune complex disease, similar to Type I. However, the immune complexes are found in the subepithelial space, and there is disruption of the glomerular basement membrane with large open areas. What is the treatment? When MPGN is associated with another condition or disease, it is usually resolved by successfully treating the associated condition or disease. However, the optimal treatment of idiopathic MPGN is not entirely known. The type of treatment will depend on the type of proteinuria that the patient has. If a patient has proteinuria that is “non-nephrotic”, then specific immunosuppressive therapy may not be necessary, as the long-term outcome is not life-threatening. However, patients with nephrotic-range proteinuria will typically be treated with steroids (Prednisone). There are some treatments that patients try if the disease does not respond to steroids, including a trial of aspirin and dipyridamole, or a combination of cyclosporine and prednisone. However, the clinical trials that have been done on these types of alternative treatments have given us very limited data. Decisions regarding treatment should be made after significant discussion between a patient and his or her nephrologist Patients with the following signs when they are first diagnosed have a worse prognosis: Nephrotic syndrome Kidney insufficiency Hypertension Crescents on kidney biopsy What is the prognosis? When MPGN is associated with another condition or disease, it is usually resolved by successfully treating the associated condition or disease. For example, if MPGN is associated with Hepatitis B or C viral infection, then MPGN tends to resolve either spontaneously or following treatment of the virus. Specific immunosuppressive therapy for MPGN is not necessary in this case. Alternatively, if the MGPN is considered idiopathic, then the outcome is not as good. Up to 50-60% of untreated patients will progress to end-stage kidney disease within 10-15 years, while 25-40% of untreated patients will continue to have normal renal function. Spontaneous remission or improvement occurs in less than 10% of cases IgA NEPHROPATHY OR BERGERS DISEASE –1RY NEPHRITIC SYNDROME WITH NORMAL S.COMPLEMENT What is IgA Nephropathy? IgA Nephropathy is a relatively common kidney disease. It affects millions of people worldwide. It is a disease that affects the filters, or glomeruli, of the kidneys. IgA is characterized by the hematuria .This blood may be visible to the naked eye or only seen under a microscope. Most people with this disease lose kidney function very slowly, or not at all. IgA Nephropathy is named for the deposits of IgA that can be seen stuck in the kidney filters when viewed under a microscope. These components normally attach themselves to infection in the body and trigger the immune response. This works to eliminate the infection. In this disease, a defective
- 25. form of IgA gets bound to another IgA molecule instead of an infection. This forms an immune complex. This immune complex can become stuck in the kidney. Here it activates the immune system just like it would if it were fighting off infection. The immune system activation causes swelling and damage to the kidney itself. However, a diagnosis of IgA Nephropathy requires a kidney biopsy. The sample of kidney can then be viewed under a microscope and the diagnosis confirmed . Clinically: Hematuria ,either recurrent gross hematuria immediately following a viral illness or as persistent microscopic hematuria .Serum creatinine is normal . Occasionally presents with acute renal failure. Prognosis good when patients have only hematuria Patients with significant proteinuria more likely to have progressive renal insufficiency Frequent world wide .In north America ,frequent among Native Americans. Diagnosis made by renal biopsy. Some patients ,more frequently children ,can have a systemic disease with disseminated vasculitis –Henoch Schoenlein purpura Biopsy— L.M.findings—glomeruli show increased mesengial matrix cellularity I.F.findings----intense granular IgA deposition ,with a mesengial pattern is observed. E.M.findings—confirms electron dense deposits in the mesengium Pathogenesis Deposition of circulating IC (( unknown antigen)) IC are found in the glomeruli and in many vessels The IgA deposits have activated the immune system and damaged the vessel wall. Therefore, red blood cells (and protein, the tiny yellow dots) are spilling out the bottom of the vessel and into the urine. Shown is a single filter in which the actual IgA deposits have been stained florescent green.
- 26. WHO IS AT RISK? IgA is an autoimmune disease . It likely has both genetic and environmental components. A person is born with a predisposition for the disease, and then some sort of “trigger,” for example an infection or food exposure, turns the disease “on ”. IgA commonly occurs in Caucasians and Asians. It is relatively uncommon in those of African descent. It is twice as common in males as females. Though it potentially affects any age group, IgA is most commonly diagnosed in early and middle adulthood. What are the symptoms? Blood in the urine, either constant or occasional, is the most common finding in people with IgA. Sometimes this blood can become visible as well. Though when it does, the urine typically appears browner or “cola” colored, rather than bright red. Bouts of visible blood in the urine from this disease often occur during or immediately after other short- term illnesses, such as an upper respiratory infection. In addition to blood in the urine, people with IgA can have protein in the urine as well. The amount of protein in the urine is generally less than 3.5g. It can sometimes result in significant leg swelling and fluid retention. IgA can be suspected from blood or protein in the urine and other symptoms. But it can only be diagnosed by a kidney biopsy. What is the treatment? This disease is common, but there is no single treatment about which all doctors agree. This is in part because of the disease tends to progress very slowly, if at all. Many of the drugs that could be used in treatment can be very harmful. It is generally accepted that blood pressure control and limiting the amount of protein in the urine are of primary importance. Both of these goals can often be accomplished with the use of two types of blood pressure medications. ACE- inhibitors and ARBs both help to reduce blood pressure. Another commonly used agent is Fish Oil. Studies do not agree on its true benefit. However, its lack of serious side-effects leads many doctors to recommend it. This disease is essentially an over-activation of the immune system. Therefore, many immunosuppressive drugs have been tried with varying success. The most widely used are steroids, given either through a needle, by mouth, or both for at least 6 months. IgA often progresses slowly. Doctors may simply follow some patients with normal renal function and minimal protein in the urine without starting any therapy at all. It is the disease’s generally slow progression that has made it difficult for doctors to decide on the one “best” treatment PROGNOSIS:
- 27. Some patients spontaneously undergo a complete remission of symptoms and never experience a loss of kidney function. More often, the symptoms will stabilize, or the disease will progress slowly. On average, at 20 years (from diagnosis), 20% of patients will have moved to end stage kidney disease. This requires either dialysis or a kidney transplant. Rarely, a more rapidly progressive type of IgA is seen on biopsy. In these patients, immediate and aggressive immunosuppression is generally needed. Kidney Transplant in IgA Nephropathy: A portion of the patients diagnosed with IgA nephropathy will eventually progress to renal failure. Fortunately, kidney transplant is a treatment option for these patients. gA Vasculitis (Formerly Henoch-Schönlein Purpura or HSP) IgA vasculitis (formerly known as Henoch Schönlein purpura) is a form of blood vessel swelling ((inflammation)) , also known as vasculitis. It affects the small vessels called capillaries in the skin and the kidneys. The swelling is due to an abnormal response of the immune system. This is due to the immune system product called IgA immunoglobulin. What does it look like (under the microscope)? Skin samples under a microscope show proteins IgA and C3 deposited in the blood vessel walls. In the kidney, IgA vasculitis (Henoch Schönlein purpura) is characterized by IgA deposits in a part of the glomerulus . These deposits can be seen under a microscope. The pathologist uses a special staining called immunofluorescence. The deposits will give a fluorescent glow under the microscope.
- 28. The pathologist can also white blood cells, and abnormal cell growth in some parts of the filter. Sometimes the pathologist will see the development of cell growths called crescents, named for their moon-like shape use Light microscopy which magnifies the kidney by 10 to 100 times its original size. This can show a wide range of changes in the kidney filter. These may range from increased cells in the filtering area, increase in. WHO IS AT RISK? IgA vasculitis has no known cause. It occurs most often in the spring. It frequently follows an infection of the throat or the respiratory tract. It seems to represent an unusual reaction of the body's immune system. This is in response to this bacterial or viral infection. Aside from infection, certain medications can also trigger the condition. IgA vasculitis occurs most commonly in children. People of all age groups can be affected. What does it affect? It affects the skin, joints, bowels and the kidneys. Infrequently, problems in other areas of the body, such as the nerves, brain and lungs may occur. Kidney -----------33% child, 665 adults ,Red or tea colored urine, weight gain, swelling on legs ,proteinuria ,azotemia. Joints -----------arthralgias and periarticular edema ((2/3)) --Joint pain and swelling of ankles , knees , wrists and elbows Skin -----------Rash in buttocks and legs, appearing as red or purple spots,nonblanching ,urticarial ,purpuric papules may become confluent --- leukocytoclastic vasculitis Gastrointestinal Tract------------Abdominal pain (2/3 of the cases) may precede the rash , nausea, vomiting, constipation or diarrhea, periumbilical pain Major complication --bowel obstruction ,intussuption , blood in the stools Lungs -------------Cough, coughing up blood What are the symptoms? IgA vasculitis usually causes a skin rash most prominent over the buttocks and behind the lower legs. Purpura It could also result in joint pain and swelling (arthritis). There is sometimes fever and cramping pain in the abdomen. The joints that are usually affected are the ankles and the knees. Swelling of the blood vessels in the kidneys can cause blood and/or protein leakage into the urine. Serious kidney complications are uncommon but can lead to advanced kidney disease. Symptoms usually last about a month. How is it diagnosed?
- 29. No single laboratory test can confirm IgA vasculitis. Certain tests can help detect the illness. Urine and blood tests for casts and kidney function can detect the presence of IgA vasculitis. Samples of the skin or kidneys can be used to diagnose vasculitis. Special stainings can be used to find the abnormal immune system product (IgA) in the blood vessels of the areas involved. What is the treatment? There is no specific treatment for IgA vasculitis. IgA vasculitis is generally a mild illness that resolves spontaneously. However, when it is severe it can cause serious problems in the kidneys and bowels. The treatment of IgA vasculitis will depend on what is most significantly affected. 1. Joint pain can be relieved by NSAIDS as aspirin or ibuprofen 2. Some patients require corticosteroid medications, prednisone or prednisolone. This is especially true for those with significant abdominal pain or kidney disease. 3. With more severe kidney disease,glomerulonephritis or nephritis. Cyclophosphamide (Cytoxan), azathioprine (Imuran), or mycophenolate mofetil (Cellcept) have been used to suppress the immune system. 4. Infection, if present, can require antibiotics. PROGNOSIS: The outlook for IgA vasculitis is generally excellent. Nearly all patients have no long- term problems. The kidney is the most serious organ involved. Some patients might have serious long-term kidney damage. Rarely, patients will experience a bowel obstruction. Surgery may be necessary to correct this. The chance of the disease coming back is low but can occur. It is usually in the form of skin rash, that comes back a few months to a year after symptoms of IgA vasculitis begin. IgA vasculitis in adults is generally more severe than in children. Adults have more severe kidney involvement. They may need more aggressive treatment. RAPIDLY PROGRESSIVE GLOMERULONEPHRITIS (( CRESENTRIC GN )) 1. TYPE I RPGN ( ANTI-GBM ANTIBODY ) Idiopathic Good pasture syndrome 2. TYPE II RPGN ( IMMUNE COMPLEX ) Idiopathic Post infectious SLE Henoch –Schonlein purpura Others 3. TYPE III RPGN ( PAUCI IMMUNE ) ANCA associated Idiopathic Wegener granulomatosis Polyarteritis nodosa /Microscopic polyangitis
- 30. Thin Basement Membrane (TBM) What is Thin Basement Membrane Disease? TBM disease (also known as benign familial hematuria and thin basement membrane nephropathy) is, along with IgA nephropathy, the most common cause of blood in the urine without any other symptoms. The only abnormal finding in this disease is a thinning of the basement membrane of the glomeruli (filters) in the kidneys. Thin basement membrane disease is a type of nephritic syndrome. It is hereditary and usually transmitted in autosomal dominant fashion. Not all genetic mutations have been characterized, but in some families with thin basement membrane disease there is a mutation in the type IV collagen α4 gene. Prevalence is estimated to be 5 to 9%. What does it look like (under the microscope)? Thin basement membrane disease is diffuse thinning of the glomerular basement membrane from a width of 300 to 400 nm in normal subjects to 150 to 225 nm. The glomerular basement wall in patients with TBM disease appears thinner. The image below is taken with an electron microscope. On the left shows a healthy kidney filter basement wall, and on the right shows a basement wall in a person with TBM disease CLINICALLY Most patients are asymptomatic and are incidentally noted to have microscopic hematuria on routine urinalysis, although mild proteinuria and gross hematuria are occasionally present. Patients with TBM usually have normal blood pressure and normal kidney function. Mild protein in the urine (less than 1.5g/day) and high blood pressure are seen in a small group of patients. Renal function is typically normal, but a few patients develop progressive renal failure for unknown reasons.Recurrent flank pain, similar to that in IgA nephropathy, is a rare manifestation. Diagnosis is based on family history and findings of hematuria without other symptoms or pathology. Renal biopsy is unnecessary but is often done as part of a hematuria evaluation. Early on, thin basement membrane disease may be difficult to differentiate from hereditary nephritis because of histologic similarities.
- 31. Long-term prognosis is excellent, and no treatment is necessary in most cases. Patients with frequent gross hematuria, flank pain, or proteinuria (eg, urine protein/creatinine ratio of > 0.2) may benefit from ACE inhibitors or angiotensin receptor II blockers, which may lower intraglomerular pressure. LUPUS GN What is lupus nephritis? Lupus nephritis is kidney inflammation caused by systemic lupus erythematosus (SLE or lupus). SLE is an autoimmune disease—a disorder in which the body’s immune system attacks the body’s own cells and organs. Up to 60 percent of people with SLE are diagnosed with lupus nephritis, which can lead to significant illness and even death. What are the symptoms of lupus nephritis? The symptoms of lupus nephritis may include high blood pressure, foamy urine, and edema— swelling, usually in the legs, feet, or ankles and less often in the hands or face. Kidney problems often develop at the same time or shortly after lupus symptoms appear and can include: Joint pain or swelling Muscle pain Fever with no known cause Red rashes, often on the face, which are also called butterfly rashes . How is lupus diagnosed? Lupus nephritis is diagnosed through urine and blood tests and a kidney biopsy A. Urine R/E When blood or protein is found in the urine. B. RFT---- the serum creatinine level is abnormally high. This can result in a decreased Glomerular Filtration Rate (GFR). C. A biopsy is the only test which can diagnose lupus nephritis. The test can confirm a diagnosis of lupus nephritis, determine how far the disease has progressed, and guide treatment. The American College of Rheumatology recommends biopsies for all people with evidence of active lupus nephritis that has not been previously treated. Once you have a biopsy, the sample is then identified based upon the degree and pattern of swelling and damage. There are six classes of the disease. Table 1: The 2003 International Society of Nephrology and International Pathology Society Classification of lupus nephritis Class I: Minimal mesangial lupus glomerulonephritis (LGN) Class II: Mesangial proliferative LGN Class III: Focal LGN (< 50% glomeruli) Class IV: Diffuse LGN (> 50% glomeruli) Class IV-S: Predominantly segmental Class IV-G: Predominantly global Class V: Membranous LGN Class VI: Advanced sclerotic LGN (> 90% sclerotic glomeruli) Why are these classes important? There are several treatment choices for people with lupus nephritis. Some of these treatment options are considered “aggressive.” They also have side effects which may not be appropriate for individuals with certain forms of lupus nephritis. The classes were based on several factors that help doctors discuss the best treatment options and outlook for people with lupus nephritis. i. Class I: Mild disease with small amount of swelling ii. Class II: Still fairly mild disease but more swelling than Class I
- 32. iii. Class III : Moderate degree of swelling < 50% of the (glomeruli) affected iv. Class IV : Severe degree of swelling with > 50% glomeruli affected v. Class IV-S: Of the affected filtering unit, < ½ of it is affected by swelling vi. Class IV-G: Of the affected filtering unit, most of it is affected by inflammation vii. Class V: Most of the swelling is confined to the outer layer surrounding the filter unit viii. Class VI : Most of the filter units show scarring What does lupus look like in a biopsy? The kidney filter of a patient with lupus will show deposits in the kidney tissue. The deposits are made up of proteins turned on to help the kidney protect itself. In this image, these deposits are pointed out with arrows and are dark gray here. There are many of them in this image collecting along the walls of the inner layer of the filter
- 33. How is lupus treated? The treatment of lupus can be complex, and should always. Doctors use a combination of approaches to try to reduce the symptoms of the disease without causing negative side effects from the treatment. Lupus nephritis is treated with medications that suppress the immune system, so it stops attacking and damaging the kidneys. Standard treatment includes a corticosteroid, usually prednisone, to reduce inflammation in the kidneys. An immunosuppressive medication, such as cyclophosphamide or mycophenolate mofetil, is typically used with prednisone. The goal of the treatment is to reduce the swelling to protect organs from damage without harming the immune system and allowing other infections to spread. Exact treatment depends on: i. The type of blood vessel swelling ii. The severity of the disease iii. How many organ systems are affected Treatment options may include a combination of some of the following: Corticosteroids---(prednisone, methyl prednisone, or Medrol®) Hydroxychloroquine (Plaquenil®) Immunosuppressive Drugs: (cyclophosphamide, cyclosporine, tacrolimus, azathioprine, mycophenolate mofetil, or Rituximab) Controlling blood pressure to reduce increased damage to the kidneys-ACE inhibitors SUMMARY:
- 34. Lupus nephritis is kidney inflammation caused by systemic lupus erythematosus (SLE or lupus). The symptoms of lupus nephritis may include high blood pressure, foamy urine, and edema. Lupus nephritis is diagnosed through urine and blood tests and a kidney biopsy. Lupus nephritis is treated with medications that suppress the immune system, so it stops attacking and damaging the kidneys. Standard treatment includes a corticosteroid, usually prednisone, to reduce inflammation in the kidneys. An immunosuppressive medication, such as cyclophosphamide or mycophenolate mofetil, is typically used with prednisone. People with lupus nephritis that is causing high blood pressure may need to take medications that lower their blood pressure, which can also significantly slow the progression of kidney disease. In many cases, treatment is effective in completely or partially controlling lupus nephritis, resulting in few, if any, further complications. However, even with treatment, 10 to 30 percent of people with lupus nephritis develop kidney failure ANCA Vasculitis What is ANCA Vasculitis? ANCA vasculitis is an autoimmune disease. ANCAs are autoantibodies that attack the (cytoplasm) of neutrophils. ANCA =Anti-Neutrophil Cytoplasmic Autoantibody. When ANCAs attack these neutrophils, they cause the white blood cells to attack the walls of small vessels in different tissues and organs of the body. This causes vasculitis. For example, vasculitis in the skin causes red spots. In the lungs or nose it causes bleeding. In the nerves it causes tingling or weakness. In the eyes it causes redness and itching. In the kidneys vasculitis causes leaking of blood and protein into the urine and kidney failure. Autoantibodies: Most patients with ANCA vasculitis have autoantibodies specific for perinuclear (P- ANCA) or cytoplasmic (C- ANCA) antibodies. C- ANCA is usually directed against proteinase 3 (PR3) and P-ANCA is usually directed
- 35. again myeloperoxidase (MPO). What are the different types of ANCA Vasculitis? In different people, ANCA vasculitis attacks different organs. It may have different disease signs. These are used to make the diagnosis of a specific form of ANCA vasculitis. Renal limited vasculitis or ANCA glomerulonephritis: The blood vessel swelling is causing capillary swelling. No other organs are affected. Microscopic polyangiitis: The swelling is causing injury to blood vessels in multiple tissues at the same time. It can be seen in the kidneys, skin, nerves, and lungs. Granulomatosis with polyangiitis -GPA- (Formerly Wegener's granulomatosis): The swelling happens with another kind of swelling called granulomatous inflammation. This often affects the lung, sinuses, nose, eyes or ears. Eosinophilic granulomatosis with polyangiitis -EGPA- (Formerly Churg-Strauss Syndrome): There is swelling, granulomatous inflammation, as well as asthmawith eosinophilia.
- 36. What is ANCA Glomerulonephritis? ANCA can cause (neutrophils) to attack the capillaries in the (glomeruli) of the kidney leading to glomerulonephritis. The destruction of the glomerular capillaries causes blood and proteins to spill into the urine. This causes the kidney to stop functioning. Glomerulonephritis often occurs in patients with ANCA disease.
- 37. What does it affect, and what are the symptoms? Vasculitis can affect any part of the body. The symptoms of vasculitis include flu-like symptoms such as fever, body aches, joint and muscle pain. There can also be reduced appetite, and weight loss. Symptoms can appear in the particular body part that is affected by the disease. The chart below explains some common symptoms that are specific to the affected body part. Kidney Brown, tea-colored urine from blood leaking into the urine Joints Joint pain or swelling Lungs Heavy cough, often mistaken for pneumonia, coughing up blood Skin Red or purple spots , itching, hives, rash Sinus/Nose Runny nose that get worse and worse, nose pain, trouble breathing through nose Trachea Shortness of breath Gastrointestinal Tract Stomach pain, or blood in stool Eyes Red, painful eyes, blurry vision, headaches Ears Hearing problems or hearing loss
- 38. DIAGNOSIS: A combination of lab tests and physical exams to diagnose vasculitis. These tests usually focus on the area of the body that is affected. Many times patients need specialists to look at a specific area. A blood test to check for ANCA Blood and urine tests to check to see if vasculitis is affecting the kidneys Chest x-rays or CT scan to check for lung problems Endoscopic exam by an ENT to check the ears, nose, and throat A biopsy, may be taken from an affected area for a lab to look at more closely How is it treated? The treatment of vasculitis can be complicated. It should always involve specialists for each affected body system. Doctors can use different approaches to try to reduce the signs of the disease. At the same time, dangerous or uncomfortable side effects from the treatment should be minimized. The goal of the treatment is to reduce the inflammation to protect organs from damage without hurting the immune system. Exact treatment depends on: The type of vasculitis How serious the disease is How many organ systems are affected Treatment options include: A. Corticosteroids: (prednisone, methyl prednisone, or Medrol) B. Immunosuppressive Drugs: (cyclophosphamide, cyclosporine, azathioprine, mycophenolate mofetil, or Rituximab) C. Antibiotics: (trimethoprim/sulfamethoxazole) Drugs that kill foreign infections that can live in the nose or in patients with a weak immune system D. Plasmapheresis: A treatment that removes the ANCA from the blood. This treatment is usually only for patients with bleeding in the lungs or kidney failure. In some patients, even with treatment, involvement of the kidney with ANCA vasculitis will lead to kidney failure. Fortunately, kidney transplant is a treatment option for these patients. Will the ANCA disease come back in my kidney transplant? About 10-15% of patients will have symptoms of ANCA disease after a kidney transplant. This is called recurrent disease. Not all return symptoms affect the kidney, but some will. It is important that ANCA disease be inactive prior to getting a kidney transplant. This reduces the chance that the ANCA disease will come back after the transplant.
- 39. Generally, ANCA disease recurrence will occur between 2.5 and 4 years after transplant. But it can occur any time. Is there any treatment for ANCA disease that comes back in a transplant? Treatments are similar to those for patients with ANCA disease in their original kidneys. They include corticosteroids and immunosuppressive drugs. These are different from the ones taken to prevent kidney transplant rejection. If the ANCA disease comes back, will it cause patient to lose the kidney transplant? Recurrent ANCA disease can rarely cause loss of a transplanted kidney. If you look at all patients with ANCA disease 10 years after their transplant, about 8% of them will have lost their kidney due to recurrent ANCA disease. A patient with ANCA disease who gets a kidney transplant can expect a similar life span and kidney transplant survival as a transplant patient who has kidney failure from another disease. Anti-GBM Disease What is Anti-Glomerular Basement Membrane Disease ( Goodpasture's Syndrome)? Anti-GBM disease is the result of injury to the (capillaries) in the kidney or lung. This can be caused by autoantibodies that attack the walls of these blood vessels. In the kidneys, the capillaries that are attacked are in the glomeruli, which filter blood and make urine. These glomerular capillaries have thin membranes in their walls that are the targets of the autoantibodies. These are called anti-glomerular basement membrane (anti-GBM) antibodies. The antibodies are found moving in the serum. The antibodies are connected to a very specific basement membrane protein. Injury to glomerular capillaries causes bleeding into the urine. It can also cause spillage of blood proteins into the urine, and reduced kidney function. In the lungs, the capillaries that are attacked are in the thin walls of air sacs where oxygen enters the blood and carbon dioxide exits. Injury to these pulmonary capillaries causes lung bleeding and impaired breathing.
- 40. Anti-GBM disease that only affects the kidneys is called anti-GBM glomerulonephritis. This is a form of inflammation, which is injury to tissue caused by white blood cells (leukocytes). Anti-GBM disease that causes both kidney disease and lung disease is called Goodpasture’s syndrome. The lung disease is anti-GBM alveolar capillaritis. This is inflammation of capillaries in the air sacs of the lungs. The kidney disease is anti-GBM glomerulonephritis. Under normal conditions, a layer of cells called endothelium protects the lower membrane from moving antibodies. However, at times there is increased leakiness of the cell layer. This happens in certain types of lung injury can be caused by exposures to organic solvents or hydrocarbons, smoking, infection, cocaine inhalation, and metal dusts. The lower membrane becomes more accessible to anti- GBM antibodies. This allows them to connect to the vessel wall and cause the swelling and bleeding that signals this anti-GBM disease.
- 41. AGE and SEX: Glomerulonephritis due to Anti-GBM antibody disease is rare. It occurs in less than 1 case per million persons. It affects mostly young, white men aged 15-35. It also can affect those beginning in the late 50’s. At this age, women are more likely to be affected. It affects both sexes equally and very rarely in children. Some evidence suggests that genetics may play an important role in this disease. CLINICAL FEATURES: 60-70% of patients have both lung and kidney involvement. This is called Goodpasture’s Syndrome.((HEMATURIA & HEMOPTYSIS)) 20-40% have only kidney involvement, which is called "renal limited" anti- GBM disease Coughing up blood is the most frequent symptom when the lungs are involved. Other symptoms may include: Chills and fever Nausea and vomiting Weight loss Chest pain Bleeding may cause anemia, respiratory failure Kidney failure How is Anti-GBM diagnosed? A Chest X-ray may be done to look for bleeding or infection.
- 42. Blood and urine tests can be done to check for kidney involvement. A CBC often shows anemia A blood test that shows that Anti-Glomerular Basement Membrane Antibodies are in the blood is essential to making the diagnosis. One third of patients with Anti-GBM disease will have (ANCA) also present at some time during their disease. Bronchoscopy with cultures may be required to fully investigate the cause of the lung bleeding. A lung sample and/or kidney sample may be taken to get a definitive diagnosis. How is Anti-GBM treated? Once the diagnosis is confirmed, there are primarily three parts to treatment. 1. The antiGBM antibody is removed from the blood stream by plasmapheresis. The number of plasmapharesis treatments can vary by patient response., Most patients receive between 5-14 treatments. These can be daily or at some approved spacing over 14 to 21 days. 2.) Further antibody production is prevented by immunosuppression. Most patients are given “pulse” large dose methylprednisolone through a needle inserted into a vein for 3 days to change the immune system function. This will reduce the production of new antibody. This is then followed by daily oral steroid therapy. The oral steroid may be given for as long as 3 months. The length of time is based on disease response to therapy.
- 43. Cyclophosphamide (Cytoxan®) is the It is generally delivered through a vein in a single monthly dose. 3.) Future exposures are avoided or prevented. Avoiding potential chemical exposures that may have caused the disease is important. Shots to prevent lung infections may also be useful. Kidney Transplant in Anti-GBM Disease: When Anti-Glomerular Basement Membrane (GBM) disease involves the kidneys, it can lead to kidney failure. Fortunately, kidney transplant is a treatment option for these patients. Will the Anti-GBM Disease come back in my kidney transplant? Treatment of anti-GBM disease is focused on removing the anti-GBM antibody from the blood. Before having a kidney transplant, it is recommended that patients wait at least 6 months after finishing treatment for anti-GBM disease. Once it is sure that the disease is no longer active, transplant is very safe. The chance that the anti-GBM disease will come back in the kidney is very low. This occurs in less than 5% of patients DM NEPHROPATHY Diabetic nephropathy is glomerular sclerosis and fibrosis caused by the metabolic and hemodynamic changes of diabetes mellitus. It manifests as slowly progressive albuminuria with worsening hypertension and renal insufficiency. Diagnosis is based on history, physical examination, urinalysis, and urine albumin/creatinine ratio. Treatment is strict glucose control, angiotensin inhibition (using ACE inhibitors or angiotensin II receptor blockers), and control of BP and lipids. WHO AT RISK? Diabetic nephropathy (DN) is the most common cause of nephrotic syndrome in adults and of end-stage renal disease in the US, accounting for up to 80% of cases of the latter. The prevalence of renal failure is probably about 40% among patients with type 1 diabetes mellitus. The prevalence of renal failure among patients with type 2 diabetes mellitus is usually stated as 20 to 30%, but this figure is probably low. Renal failure is particularly common in certain ethnic groups, such as blacks, Mexican-Americans, Polynesians, and Pima Indians. Other risk factors include the following: 1) Duration and degree of hyperglycemia 2) Hypertension 3) Dyslipidemia 4) Cigarette smoking
- 44. 5) Certain polymorphisms affecting the renin-angiotensin-aldosterone axis 6) Family history of diabetic nephropathy 7) Genetic variables (decreased number of glomeruli) Renal failure usually takes ≥ 10 yr after the onset of nephropathy to develop; however, because type 2 diabetes is often present for several years before being recognized, nephropathy often develops < 10 yr after diabetes is diagnosed. PATHOPHYSIOLOGY: 3 Types of lesions: 1. Glomerular disease 2. Vascular lesions---nephrosclerosis 3. pyelonephritis Pathogenesis begins with small vessel disease. Pathophysiology is complex, involving glycosylation of proteins, hormonally influenced cytokine release (eg, transforming growth factor-β), deposition of mesangial matrix, and alteration of glomerular hemodynamics. Hyperfiltration, an early functional abnormality, is only a relative predictor for the development of renal failure. Hyperglycemia causes glycosylation of glomerular proteins, which may be responsible for mesangial cell proliferation and matrix expansion and vascular endothelial damage. The glomerular basement membrane classically becomes thickened. Each nephron has 3 parts: 1) a small blood vessel that brings in unfiltered blood, 2) a glomerulus that filters the blood and 3) a small blood vessel that returns filtered blood to the body. The earliest detectable change in glomeruli is thickening of the thin basement
- 45. membrane. Damage to this membrane causes proteins to leak from the blood into the urine which is identified in a kidney using an electron microscope . Lesions of diffuse or nodular intercapillary glomerulosclerosis are distinctive; areas of nodular glomerulosclerosis may be referred to as Kimmelstiel-Wilson lesions . There is marked hyalinosis of afferent and efferent arterioles as well as arteriosclerosis; interstitial fibrosis and tubular atrophy may be present. Only mesangial matrix expansion appears to correlate with progression to end-stage renal disease. Diabetic Nephropathy Nodules (DN) (Mesangial Cell Proliferation and Matrix Expansion) DN begins as glomerular hyperfiltration (increased GFR); GFR normalizes with early renal injury and mild hypertension, which worsens over time. Microalbuminuria, urinary excretion of albumin in a range of 30 to 300 mg albumin/day, then occurs. Urinary albumin in these concentrations is called microalbuminuria because detection of proteinuria by dipstick on routine urinalysis usually requires > 300 mg albumin/day.
- 46. Microalbuminuria progresses to macroalbuminuria (proteinuria > 300 mg/day at a variable course, usually over years. Nephrotic syndrome (proteinuria ≥ 3 g/day) precedes end-stage renal disease, on average, by about 3 to 5 yr, but this timing is also highly variable. Other urinary tract abnormalities commonly occurring with DN that may accelerate the decline of renal function include papillary necrosis, type IV renal tubular acidosis, and UTIs. In DN, the kidneys are usually of normal size or larger. HYALINOSIS Symptoms and Signs DN is asymptomatic in early stages. Sustained MICROALBUMINURIA is the earliest warning sign((30mg/day but < 300mg/day)). Within 10—15 years patients with diabetes develop overt nephropathy with MACROALBUMINURIA .This is associated with HTN. Hypertension and some measure of dependent edema eventually develop in most untreated patients. In later stages, patients may develop symptoms and signs of uremia (eg, nausea, vomiting, anorexia) earlier (ie, with higher GFR) than do patients without DN, possibly because the combination of end-organ damage due to diabetes (eg, neuropathy) and renal failure worsens symptoms. Capillary basement membrane thickening Diffuse mesangial sclerosis Nodular glomerulosclerosis Renal arteriolosclerosis and atherosclerosis Hyaline arteriolosclerosis affects both afferent &efferent arterioles. Patient develop nephritic syndrome after long standing glomerulosclerosis Nodular glomerulosclerosis is characterized by distinctive ball like deposits of a laminated matrix situated in the periphery of the glomerulus . These are PAS positive and contain trapped mesangial cells. ((KIMMELSTIEL-WILSON KIDNEY)) Diagnosis : Yearly screening of all patients with diabetes with random urine albumin/creatinine ratio. Urinalysis for signs of other renal disorders (eg, hematuria, RBC casts) The diagnosis is suspected in patients with diabetes who have proteinuria, particularly if they have diabetic retinopathy (indicating small vessel disease) or risk factors for DN. Other renal disorders should be considered if there are any of the following: 1) Heavy proteinuria with only a brief history of diabetes
- 47. 2) Absence of diabetic retinopathy 3) Rapid onset of heavy proteinuria 4) Gross hematuria 5) RBC casts 6) Rapid decline in GFR 7) Small kidney size HOW TO DETECT PROTEINURIA? Patients are tested for proteinuria by routine urinalysis; if proteinuria is present, testing for microalbuminuria is unnecessary because the patient already has macroalbuminuria suggestive of diabetic renal disease. In patients without proteinuria on urinalysis, an albumin/creatinine ratio should be calculated from a mid-morning urine specimen. A ratio ≥ 0.03 mg/mg (≥ 30 mg/g) indicates microalbuminuria if it is present on at least 2 of 3 specimens within 3 to 6 mo and if it cannot be explained by infection or exercise. Some experts recommend that microalbuminuria be measured from a 24-h urine collection, but this approach is less convenient, and many patients have difficulty accurately collecting a specimen. The random urine albumin/creatinine ratio overestimates 24-h collection of microalbuminuria in up to 30% of patients > 65 due to reduced creatinine production from reduced muscle mass. Inaccurate results can also occur in very muscular patients or if vigorous exercise precedes urine collection.For most patients with diabetes who have proteinuria, the diagnosis is clinical. Renal biopsy can confirm the diagnosis but is rarely necessary Screening: Patients with type 1 diabetes without known renal disease should be screened for proteinuria and, if proteinuria is absent on routine urinalysis, for microalbuminuria, beginning 5 yr after diagnosis and at least annually thereafter. Patients with type 2 diabetes should be screened at the time of diagnosis and annually thereafter Prognosis : Prognosis is good for patients who are meticulously treated and monitored. Such care is often difficult in practice, however, and most patients slowly lose renal function; even prehypertension (BP 120 to 139/80 to 89 mm Hg) or stage 1 hypertension (BP 140 to 159/90 to 99 mm Hg) may accelerate injury. Systemic atherosclerotic disease (stroke, MI, peripheral arterial disease) predicts an increase in mortality. TREATMENT: Prevention and awareness are very important to everyone with diabetes. 1. Urinalysis : All diabetics should have a urine test at least once every year. This test looks for the presence of the protein albumin. 2. Blood Sugar Control: Maintenance of glycosylated Hb (HbA 1c ) ≤ 7.0 Keeping blood sugar levels well controlled helps maintain kidney health. In a recent study, diabetic patients that kept their blood sugar below 150 mg/dl greatly reduced the risk of kidney disease.The American Diabetes Association recommends that blood sugars be kept between 90-130 mg/dl on an empty stomach. Blood sugar should be less than 180 mg/dl one hour after eating. 3. Blood Pressure: High blood pressure is extremely common in diabetics. It is a major cause of kidney disease. Additionally, kidney disease can make high blood pressure even higher. This creates a vicious cycle. Often, it takes multiple medications to control high blood pressure. This is especially true for
- 48. diabetics, obese patients, and the elderly. The American Diabetes Association recommends checking blood pressure twice every year. Keeping blood pressure below 130/80 is also recommended. Patients who cannot control their blood pressure with diet and exercise alone are usually prescribed blood pressure reducing medicine. This is known as an "ACE inhibitor" or an "ARB". Some experts suggest BP should be 110 to 120/65 to 80 mm Hg, particularly in patients with protein excretion of > 1 g/day; however, others claim that BP values < 120/85 mm Hg are associated with increased cardiovascular mortality and heart failure. Angiotensin inhibition is first-line therapy. Thus, ACE inhibitors or angiotensin II receptor blockers are the antihypertensives of choice; they reduce BP and proteinuria and slow the progression of DN. ACE inhibitors are usually less expensive, but angiotensin II receptor blockers can be used instead if ACE inhibitors cause persistent cough. Treatment should be started when microalbuminuria is detected regardless of whether hypertension is present; some experts recommend drugs be used even before signs of renal disease appear. Diuretics are required by most patients in addition to angiotensin inhibition to reach target BP levels. Dose should be decreased if symptoms of orthostatic hypotension develop or serum creatinine increases by more than 30%. Nondihydropyridine Ca channel blockers (diltiazem and verapamil) are also antiproteinuric and renoprotective and can be used if proteinuria does not meaningfully decrease when target BP is reached or as alternatives for patients with hyperkalemia or other contraindications to ACE inhibitors or angiotensin II receptor blockers. In contrast, dihydropyridine Ca channel blockers (eg, nifedipine, felodipine, amlodipine) do not reduce proteinuria, although they are useful adjuncts for BP control and may be cardioprotective in combination with ACE inhibitors. ACE inhibitors and nondihydropyridine Ca channel blockers have greater antiproteinuric and renoprotective effects when used together, and their antiproteinuric effect is enhanced by Na restriction. Nondihydropyridine Ca channel blockers should be used with caution in patients taking β-blockers because of the potential to worsen bradycardia. 4. Statins should be used as first-line therapy for hyperlipidemia treatment in patients with DN because they reduce cardiovascular mortality and urinary protein. Cholesterol: High cholesterol is common in diabetics. Therefore, the risk of developing kidney disease from high cholesterol is a concern. This concern makes controlling cholesterol very important. Sometimes a healthy, balanced diet is enough to control cholesterol. Sometimes medication is needed. The American Diabetes Association recommends that the LDL (bad cholesterol) be less than 100. HDL (good cholesterol) should be higher than 40. Triglycerides should be less than 150. 5. Dietary protein restriction yields mixed results. Significant protein restriction is not recommended. Evidence shows that too much or too little protein can be harmful. The American Diabetes Association recommends following USDA guidelines. Patients should consume 5-6 ounces of meat and 2-3 servings of dairy every day. The American Diabetic Association recommends that people with diabetes and overt nephropathy be restricted to 0.8 to 1.2 g protein/kg/day. 6. Smoking: Smoking worsens the progression of kidney disease. Quitting smoking is extremely difficult. There are several treatments which have been proven to help people quit.
- 49. 7. Weight loss and Exercise: Being overweight contributes to kidney disease by making diabetes harder to control. It raises blood pressure and causes scarring in the kidneys. Weight loss often improves blood sugars. It also decreases the number of medications necessary to control blood pressure. 8. Body Mass Index (BMI) is a scale that uses weight and height to determine whether someone is overweight. A BMI 25-30 indicated that someone is overweight. An obese person has a BMI over 30. Planning a diet and exercise program to reach a BMI of less than 25 will greatly reduce diabetic risk factors 9. Kidney transplantation with or without simultaneous or subsequent pancreas transplantation is an option for patients with end-stage renal disease. The 5-yr survival rate for patients with type 2 diabetes receiving a kidney transplant is almost 60%, compared with 2% for dialysis-dependent patients who do not undergo transplantation . Renal allograft survival rate is > 85% at 2 yr Diabetic nephropathy is very common, asymptomatic until late, and should be considered in all patients with diabetes. Periodically screen all patients with diabetes with urinalysis and, if proteinuria is absent, albumin/creatinine ratio calculated from a mid-morning urine specimen. Treat BP aggressively, usually beginning with angiotensin inhibition. Control glucose to maintain HbA 1c at ≤ 7.0. Myeloma Kidney What is Multiple Myeloma? Multiple Myeloma is a blood cancer of the plasma cells.(( Plasma cells are immune cells that normally make special proteins, called antibodies, to fight off disease. These antibodies are part of the body’s defense system to neutralize infections that invade the blood stream)). Patients who have multiple myeloma make plasma cells that are abnormal. These plasma cells do not make normal antibodies anymore, but instead make too much of one kind of protein-paraprotein. When this happens, the levels of these proteins in the blood become higher than normal. The abnormal plasma cells and the abnormal proteins cause the major symptoms of multiple myeloma: bone disease, anemia, renal failure, increased risk of infection, and high levels of calcium. What is Myeloma Kidney? Kidney failure is a common complication of multiple myeloma. When first diagnosed, as many as 20-40% of patients with multiple myeloma will have some amount of kidney failure. Multiple myeloma can affect the kidney in several ways. It can affect 1. The filter (glomerulus) 2. The tubules (pipes)-- myeloma kidney ((cast nephropathy )) 3. The tissue of the kidney itself (interstitium). The effect of multiple myeloma on the glomerulus (filter) due to light chain, heavy chain deposition, and amyloidosis.
- 50. How does Multiple Myeloma affect the kidneys? The tubules are the pipes through which filtered blood ultimately becomes urine and exits the body as waste. The blood passes through the glomeruli and then enters the tubules (pipes). The abnormal proteins that are made by the plasma cells in patients with multiple myeloma float around in the blood stream. The blood passes through the filters in the kidneys and these abnormal proteins enter the tubules. These abnormal proteins then travel through the tubules and can join up with another type of protein normally present in the urine, Tamm Horsfall protein. If these two proteins join together they become too big to pass on through the tubules and therefore cannot exit the kidney in the form of urine. This combination of proteins results in large casts that block the tubules inside the kidney. These tubules are just like pipes that carry water, when they get blocked fluid cannot flow through. These blockages lead to kidney damage. In addition to blockages, these casts cause an inflammatory reaction in the tissue of the kidney around them. When kidney failure occurs due to these blockages, we call this cast nephropathy or myeloma kidney. The tubules of the kidney can also be damaged simply due to the toxic effects of these filtered proteins. This can lead to abnormal kidney function even in the absence of cast formation. However, myeloma kidney is by far the most common manifestation of kidney disease in patients with multiple myeloma.
- 51. Three distinct syndromes account for most cases of Ig-mediated kidney disease but virtually all nephropathologic syndromes have been observed. Panel A shows amyloid. (i) Amyloid fibrils consisting of monoclonal Ig and serum proteins appear here as pink material disrupting glomeruli architecture. (ii) (ii) Amyloid is visible on electron microscopy as 7- to 12-nm fibrils. Panel B shows MIDD. Monoclonal light chains kappa (1) or without evidence of lambda (ii) and/or heavy chains (IgG), deposit along glomerular (iii) and tubular basement membranes (iv), altering the glomerular structure and causing dose- dependent proximal tubular toxicity. Panel C shows cast nephropathy. Filtered monoclonal Ig, Tamm-Horsfall, and other proteins form casts, which obstruct tubules and collecting ducts. Casts can rupture and result in interstitial inflammation. Panel D shows interstitial inflammation. Inflammation also results from the processing of filtered monoclonal light chains, which induces NF-κB and other signaling pathways leading to cytokine-mediated inflammatory infiltrate (shown here with a Trichrome stain) and subsequent matrix deposition and fibrosis. Panel E shows glomerular crescent. Shown here is a glomerular crescent in a patient with Waldenström macroglobulinemia productive of IgMλ and amyloidosis What does it look like (under the microscope)? By biopsy ,in cast myeloma kidney, the tubules full of proteins that blocks the inside of the tubule. The glomeruli (filters) of the kidney are typically not affected in cast nephropathy and usually appear normal. How is at risk? UKNOWN. It is a rare disease and affects only about 1 in 4,000 people. Each year about 13,000-20,000 people will be diagnosed with this disease. There are some studies that show people who have been exposed to certain toxins like radiation, benzene, herbicides, insecticides, and organic solvents are more at risk than the general population. However, many people develop multiple myeloma without any exposure to these agents. The age --- 50s and 60s. It is unknown why people develop this disease and it is not possible to predict who will develop it. Not all patients with multiple myeloma will develop myeloma kidney, generally about 30-50% of patients develop this problem. There are things that will make a patient with multiple myeloma more at risk to develop myeloma kidney. Dehydration, therapy with
- 52. furosemide (a fluid pill), high blood levels of calcium, and high levels of sodium in the urine all can lead to increased formation of these casts. What are the symptoms? The symptoms of multiple myeloma are typically fatigue, bone pain, and infections. This is because multiple myeloma causes anemia, destruction of the bones, and decreased production of normal antibodies (proteins) that fight infection. The destruction of the bones due to multiple myeloma can often lead to fractures of the bone that occur with little or sometimes no trauma. Often, though, the signs of kidney dysfunction will be first discovered on lab work done for another medical reason. Lab results could show increased level of creatinine, or increased amount of protein in the urine. People who develop advanced kidney disease will have symptoms related to kidney failure including nausea, itching, confusion, and fatigue. How is it diagnosed? In order to diagnose myeloma kidney, a biopsy needs to be done. In cast nephropathy---- tubular casts in the distal nephron, often with accompanying interstitial nephritis. In MIDD, tubular and glomerular basement membranes are thickened by refractile precipitates that are granular and dense on electron microscopy. Glomerular nodules resembling the Kimmelstiel-Wilson lesion of diabetic nephropathy may be present and cause the nephrotic syndrome. In AL amyloidosis, the tubular basement membranes are typically of normal thickness but the Congo red stain is positive, with characteristic green birefringence under polarizing microscopy. Electron microscopy demonstrates organized deposits of nonbranching amyloid fibrils, 7 to 10 nm in diameter These include blood tests, urine tests, x-rays of the bones, and a bone marrow biopsy. The blood tests and urine tests can detect the abnormal proteins that are made by the plasma cells. The x-rays of the bones look for lesions in the bones caused by the multiple myeloma. The bone marrow biopsy will find the abnormal plasma cells inside the bones. What is the treatment? The treatment for the kidney disease associated with multiple myeloma depends upon treating the myeloma itself. Patients with multiple myeloma are treated with chemotherapy and/or bone marrow transplant. Bone marrow transplant is only for patients who have good mobility and function and do not have severe kidney, liver, or heart disease. For chemotherapy, the most common regimen involves a combination of prednisone, thalidomide, and melphalan. Chemotherapy can help reduce the production of the abnormal proteins by the plasma cells, which is very important for patients with myeloma kidney. By reducing the abnormal protein in the blood, the kidney will have a chance to recover. The role of stem cell transplantation, plasma exchange, and kidney transplantation in the management of patients with paraprotein- related kidney disease continues to evolve. In addition to chemotherapy to treat the multiple myeloma, there are a few other things that can help patients with myeloma kidney.
- 53. A. Keeping hydrated is very important, because being dehydrated can lead to more cast formation. Therefore, drinking 2-3L of water a day is recommended. B. Avoiding NSAIDs (like ibuprofen) and diuretics (like furosemide) are important because these medications cause more cast formation. C. Treating high blood levels of calcium is important so that the high calcium levels do not filter through the kidney and make cast formation worse. High calcium levels are usually treated with medications such as pamidronate and zolendronic acid. D. Finally, patients with multiple myeloma and especially those with myeloma kidney should not get IV contrast. What are the chances that I will get better? The prognosis for multiple myeloma depends in large part on if the kidney is affected and how badly. Patients who have kidney dysfunction will have an average survival of 20 months (slightly less than 2 years). Those patients without kidney dysfunction will have an average survival of 40 months (between 3 and 4 years). Among all patients, response to chemotherapy is very important as well. Patients whose kidney function improves with chemotherapy have an average survival of 3 years. Those patients whose kidney function does not improve with chemotherapy will only live an average of 10 months. OTHER ENTITY OF MM IN KIDNEY: A. Glomerulonephritis may occur, of either a membranoproliferative, diffuse proliferative, crescentic, or cryoglobulinemic variety. B. Nephrotic syndrome may result from an Ig-induced minimal change or membranous lesion. C. Renal limited thrombotic microangiopathy can result directly from monoclonal Ig-induced endothelial injury or after chemotherapy . D. IgA myeloma can rarely result in Henoch-Schonlein purpura and IgA nephropathy. E. Patients with circulating monoclonal IgM can develop kidney injury from hyperviscosity or when deposits composed of monoclonal IgM occlude glomerular capillaries. F. Crystalline inclusions in the proximal tubule consisting of monoclonal Ig can .0result in a mild tubulointerstitial nephritis or the Fanconi syndrome, which is often indolent and may not require systemic therapy The reversible, first in class proteasome inhibitor bortezomib is a U.S. Food and Drug Administration–approved small molecule boronic acid–derived peptide that targets protein handling mediated by the ubiquitin proteasome pathway. Bortezomib has emerged along with high-dose dexamethasone as among the most effective approaches for treating myeloma when associated kidney injury is present. It is also now well established as therapy for relapsed myeloma and has recently received approval for initial therapy.Rapidly acting, it is characterized by a median time to best response of approximately 30 days in previously treated patients. As malignant plasma cells synthesize and assemble large quantities of Ig, they are particularly susceptible to proteasome inhibitors, which induce myeloma cell apoptosis in part by interfering with protein handling. Bortezomib also inhibits the NF-κB and MAPK pathways, which
- 54. leads directly to myeloma cell apoptosis while also disrupting myeloma-stromal cell interactions and tumoral angiogenesis. The proinflammatory cascade is mediated by mitogen-activated protein kinase (MAPK) and nuclear factor-κB (NF-κB) pathways. Importantly, by inhibiting the NF-κB and MAPK pathways, bortezomib mitigates the inflammatory state induced in proximal tubule cells by excessive light chain handling and so may protect these cells from apoptosis by up-regulating heat shock and other survival-associated proteins. In contrast to traditional agents whose toxicity increases in renal impairment, the antimyeloma effects and safety profile of bortezomib appear unchanged in this setting, and renal dose adjustment is therefore not required. When combined in various regimens with dexamethasone, melphalan, doxorubicin, or thalidomide, 40% to 50% of patients who respond to therapy will experience significant recovery of renal function within 2 to 3 weeks. Improvement in renal function appears to precede the expected antiplasma cell effects of bortezomib, possibly reflecting anti- inflammatory properties of the agent. To improve efficacy of dexamethasone, it is often combined with thalidomide or its potent, newer derivative, lenalidomide, which interferes with myeloma cell growth, disrupts myeloma and bone marrow stromal cell interactions, down-regulates promyeloma cytokines, and up-regulates antimyeloma T-cell activity. Although the pharmacokinetics of thalidomide appear unaffected by renal function, hyperkalemia has been reported in the setting of renal dysfunction. Dose reduction is required with lenalidomide, as the drug's clearance falls significantly in advanced CKD. Importantly, patients with creatinine in excess of 2.5 mg/dL have been excluded from lenalidomide trials, and patients with lesser degrees of renal dysfunction experience more adverse events, particularly myelosuppression. Fibrillary and Immunotactoid Glomerulopathies fbrillary and immunotactoid glomerulopathies are rare conditions defined pathologically by organized deposition of nonamyloid microfibrillar or microtubular structures within the renal mesangium and basement membrane. Fibrillary and immunotactoid glomerulopathies are thought by some experts to be related disorders. They are found in about 0.6% of renal biopsy specimens, occur equally in men and women, and have been described in patients ≥ 10 yr. Average age at diagnosis is about 45. Mechanism is unknown, although deposition of immunoglobulin, particularly IgG κ and λ light chains and complement (C3), suggests immune system dysfunction. Patients may have accompanying paraproteinemia, cryoglobulinemia, plasma cell dyscrasia, hepatitis C infection, or SLE, or they may have a primary renal disease without evidence of systemic disease. CLINICAL: All patients have proteinuria, > 60% nephrotic range. Microscopic hematuria ((60%)); hypertension, in about 70%. Slightly > 50% have renal insufficiency at presentation. Diagnosis : Renal biopsy Diagnosis is suggested by laboratory data and confirmed by renal biopsy. If nephrotic syndrome is present, testing is done as for other cases of nephrotic syndrome. Urinalysis usually shows features of nephritic and nephrotic syndromes. Serum C3 and C4 are usually measured and are occasionally decreased. Light microscopy of a
- 55. biopsy specimen shows mesangial expansion by amorphous eosinophilic deposits and mild mesangial hypercellularity. Various other changes may be present on light microscopy (eg, crescent formation, membranoproliferative patterns). Congo red staining is negative for amyloid. Immunostaining reveals IgG and C3 and sometimes κ and λ light chains in the area of the deposits. Electron microscopy shows glomerular deposits consisting of extracellular, elongated, nonbranching microfibrils or microtubules. The diameter of the microfibrils and microtubules varies from 20 to 30 nm for fibrillary glomerulonephritis and from 30 to 50 nm for immunotactoid glomerulonephritis, in contrast to the 8 to 12 nm fibrils that occur in amyloidosis. Some experts distinguish immunotactoid from fibrillary glomerulopathy by the presence of microtubular (as opposed to smaller microfibrillar) structures in the deposits; others distinguish them by the presence of a related systemic illness such as a paraproteinemia, cryoglobulinemia, or SLE in immunotactoid glomerulonephritis. Fibrillary Glomerulopathy (Mesangial Proliferation) Fibrillary Glomerulopathy (IgG Deposition) Fibrillary Glomerul opathy (Fibrils) Immunotactoid Glomerulopathy Prognosis :
- 56. The condition is usually slowly progressive with renal insufficiency, progressing to end-stage renal disease in 50% of patients within 2 to 4 yr. A more rapid decline is predicted by the presence of hypertension, nephrotic-range proteinuria, and renal insufficiency at presentation. Treatment Evidence is lacking, but consider ACE inhibitors or angiotensin II receptor blockers, immunosuppressants, and/or corticosteroids Evidence to support specific treatments is lacking although ACE inhibitors and angiotensin II receptor blockers may be used to reduce proteinuria. Immunosuppressants have been used based on anecdotal evidence but are not a mainstay of therapy; success may be greater with corticosteroids when serum complement is decreased. The disorder may recur after transplantation. AL Amyloidosis AL Amyloidosis (also called “primary” amyloidosis) is a blood illness in which a special protein builds up in various parts of the body. This protein, called “M-protein,” is actually made up of pieces from immunoglobulins (also called antibodies) which are naturally in the body and fight off infection. In the case of people with amyloidosis, too many of these disease fighting pieces are present in blood flow. They can get stuck in almost any organ in the body, such as the brain, the lungs, the liver, the heart, the skin, or the kidneys. As these proteins build up, they begin to get in the way of the job of whichever organ they are in. Although AL amyloidosis can be assumed from many of its different symptoms , the only way to know for sure that it is there is to analyze the cells with a biopsy. Kidney, amyloidosis happens when the irregular proteins began to get stuck in the kidneys. As the amyloid builds up, the kidneys are no longer able to work properly leading to kidney failure. Eventually kidney failure can also cause problems with low red blood cell count, high blood pressure, and fluid buildup. What does it look like?
- 57. Glomerulus affected by AL Amyloidosis In the affected filter on the right, almost all of these loops have flattened because of all the built up M-protein. Shown above are two glomeruli, or kidney filters, as they look under a microscope. The normal filter is on the left, and the filter damaged by this disease is on the right. See that in the normal filter, there are many open “loops” scattered throughout- these are all small blood vessels seen in a small piece cut from the kidney. This time a “stain” has been added that turns the damaged cells bright green. This is another stain that is used in finding disease, called “Congo Red”. This stain turns “bright apple green” when it touches the sick cells. WHO AT RISK? We don’t yet know why some people get AL amyloidosis, even though 1,000-3,000 new cases are found each year in the US. About 2/3 of these patients are male, and almost all of them are over the age of 40. Although this type of amyloidosis can occur by itself, it often happens with other blood disorders, such as multiple myeloma and