Download as PDF, PPTX









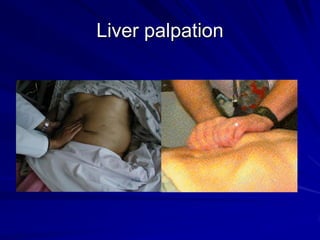


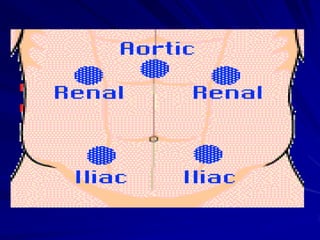

This document provides instructions for performing an abdominal examination, including techniques for palpation, percussion, and auscultation. It describes how to palpate the abdominal quadrants and specific organs like the liver and spleen. Instructions are given for percussion of the liver and checking for shifting dullness. The fluid thrill test and listening for bowel sounds and bruits are also outlined. The goal is to examine the abdominal contour, feel for masses or swelling, and check the size and position of internal organs.








![ABDOMINAL EXAMINATION Presentation[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/abdominalexaminationpresentation1-240105120242-b6318479-thumbnail.jpg?width=640&height=640&fit=bounds)


























































