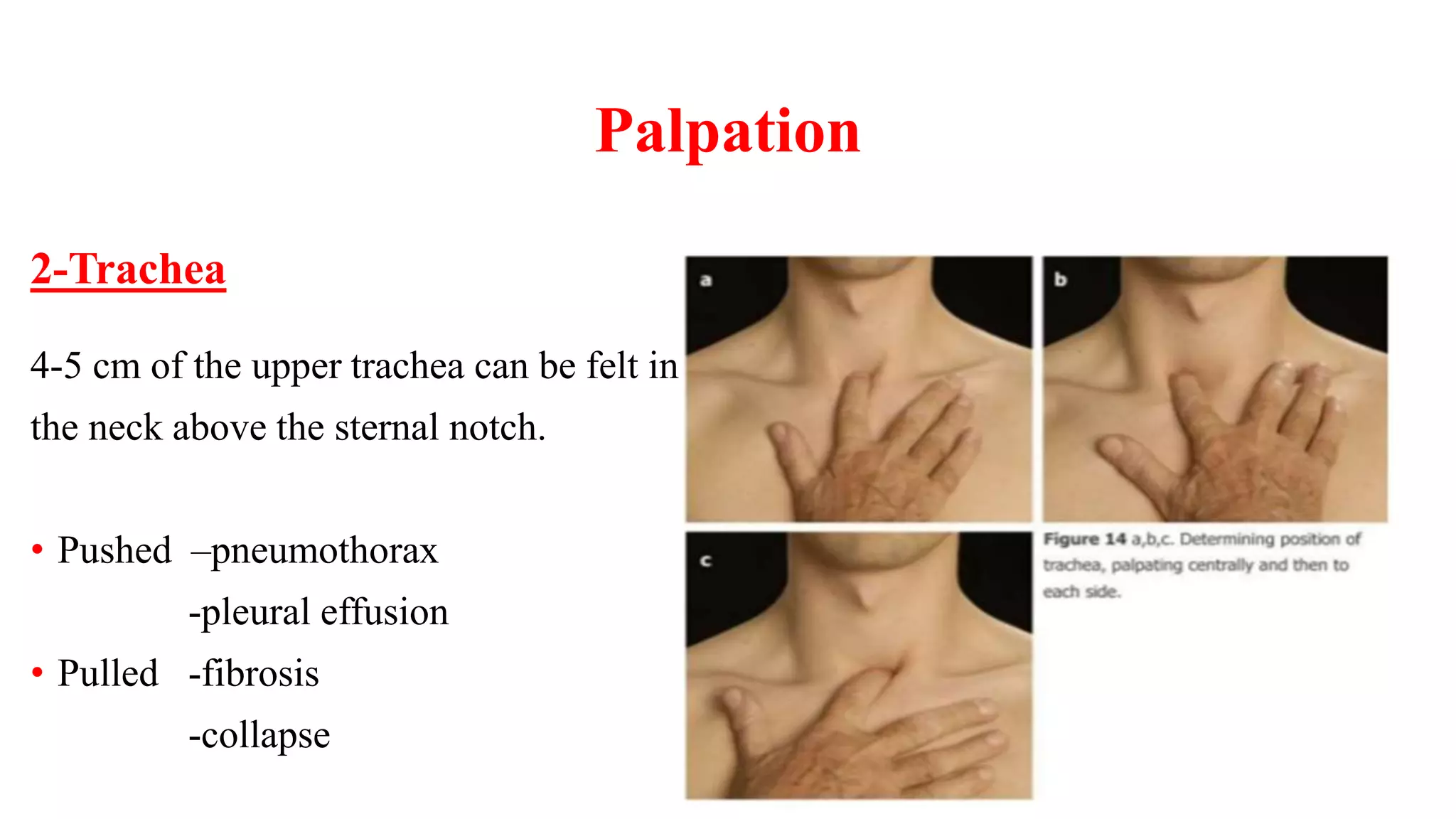
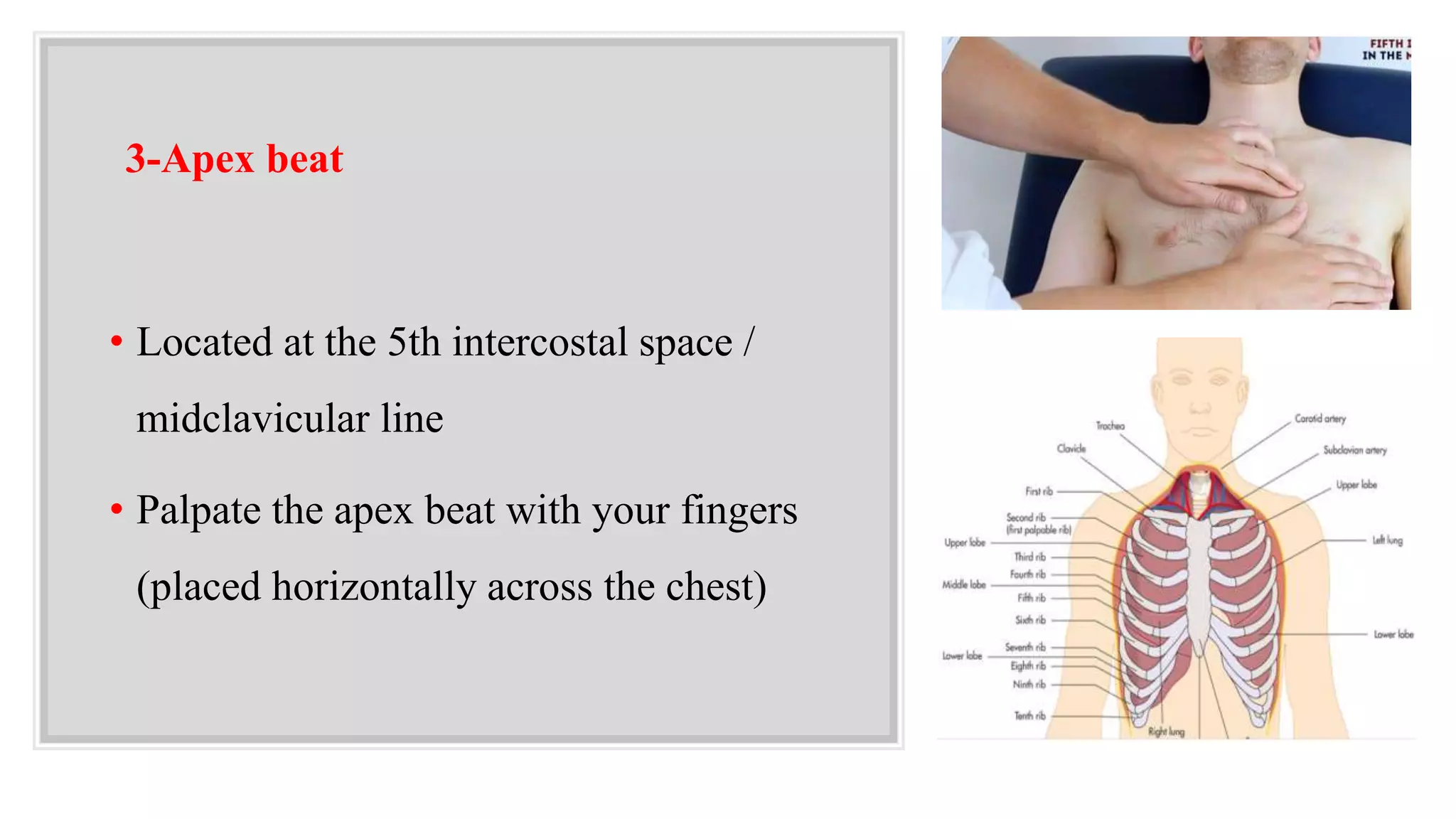
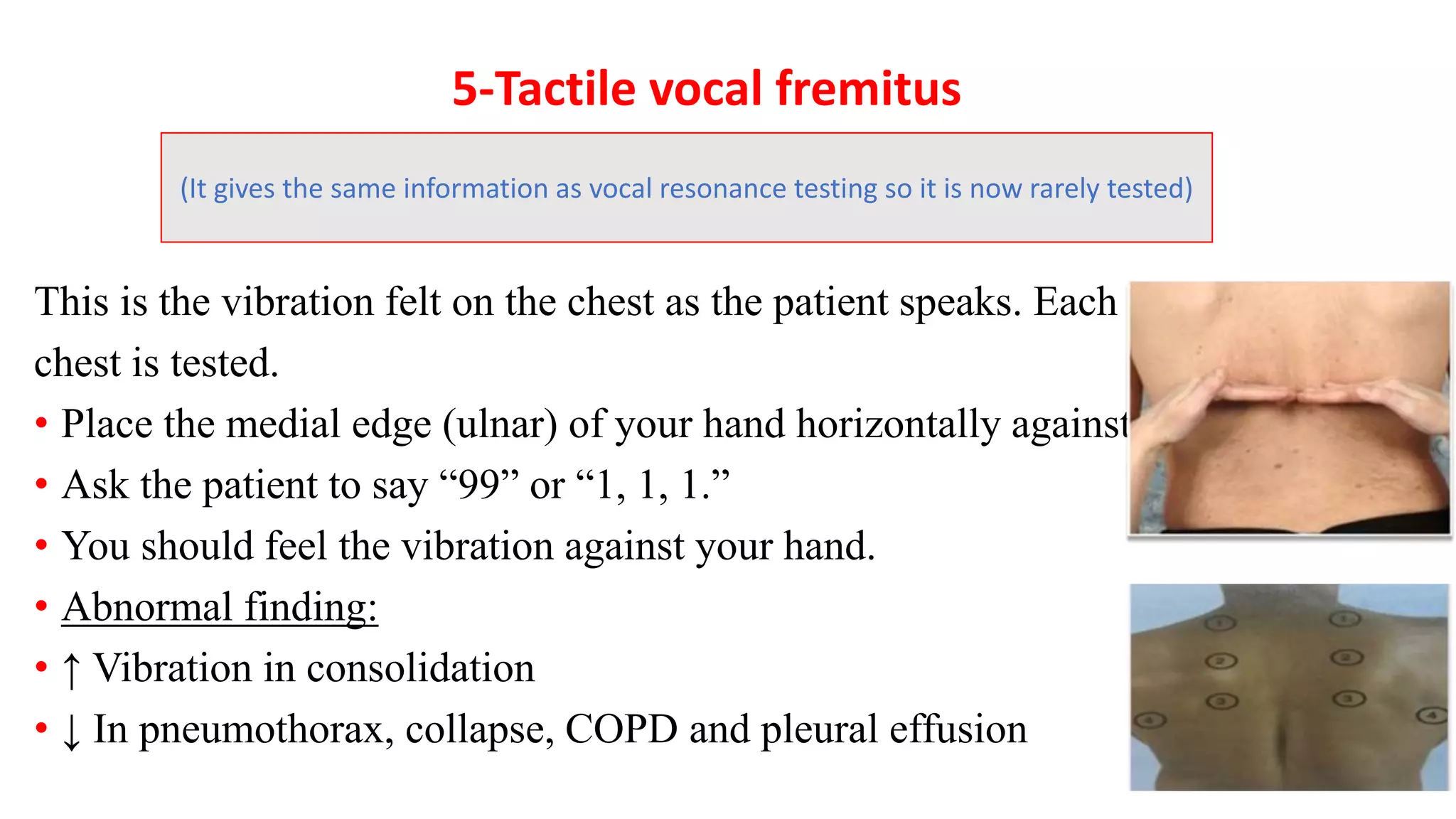
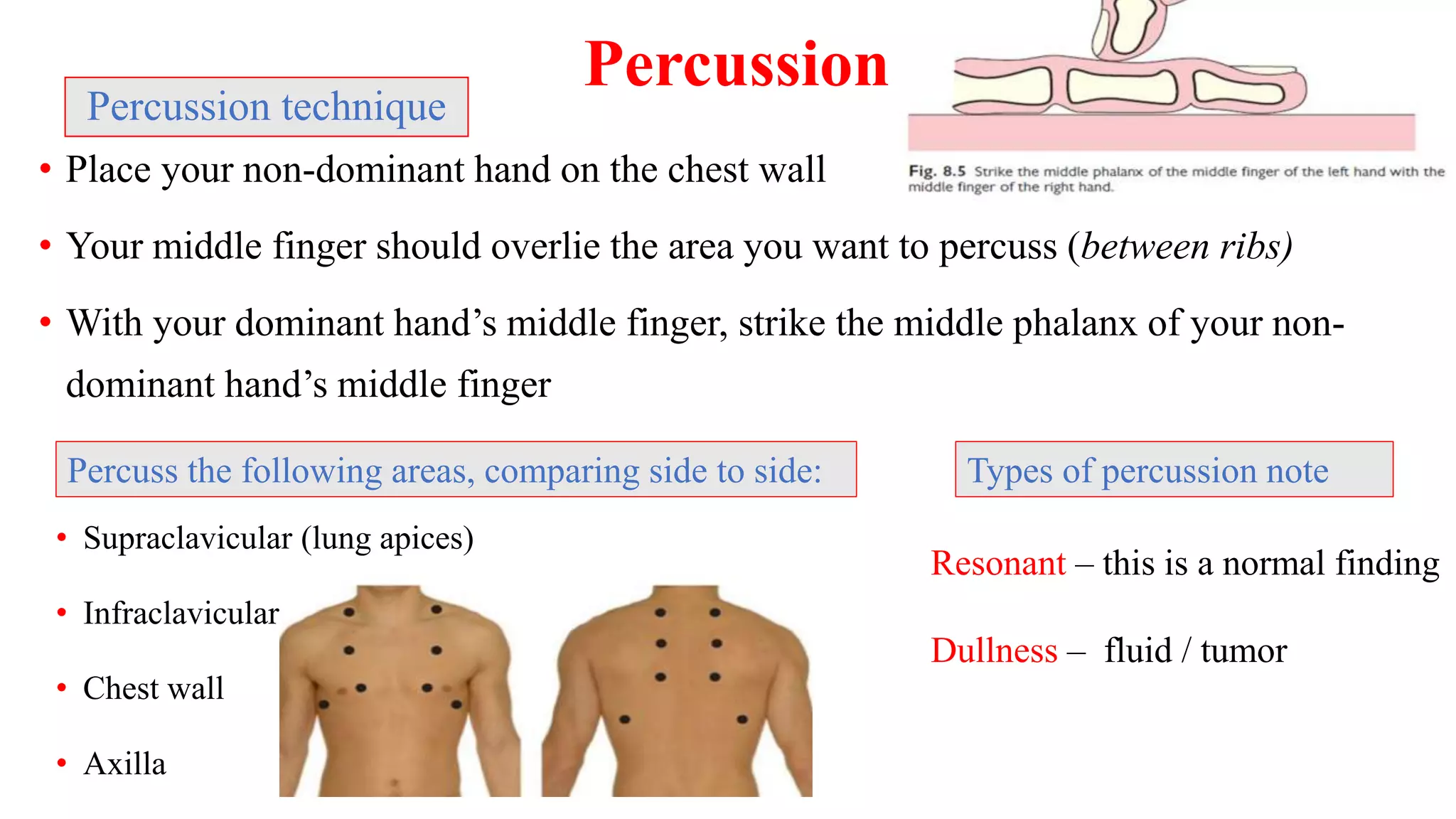
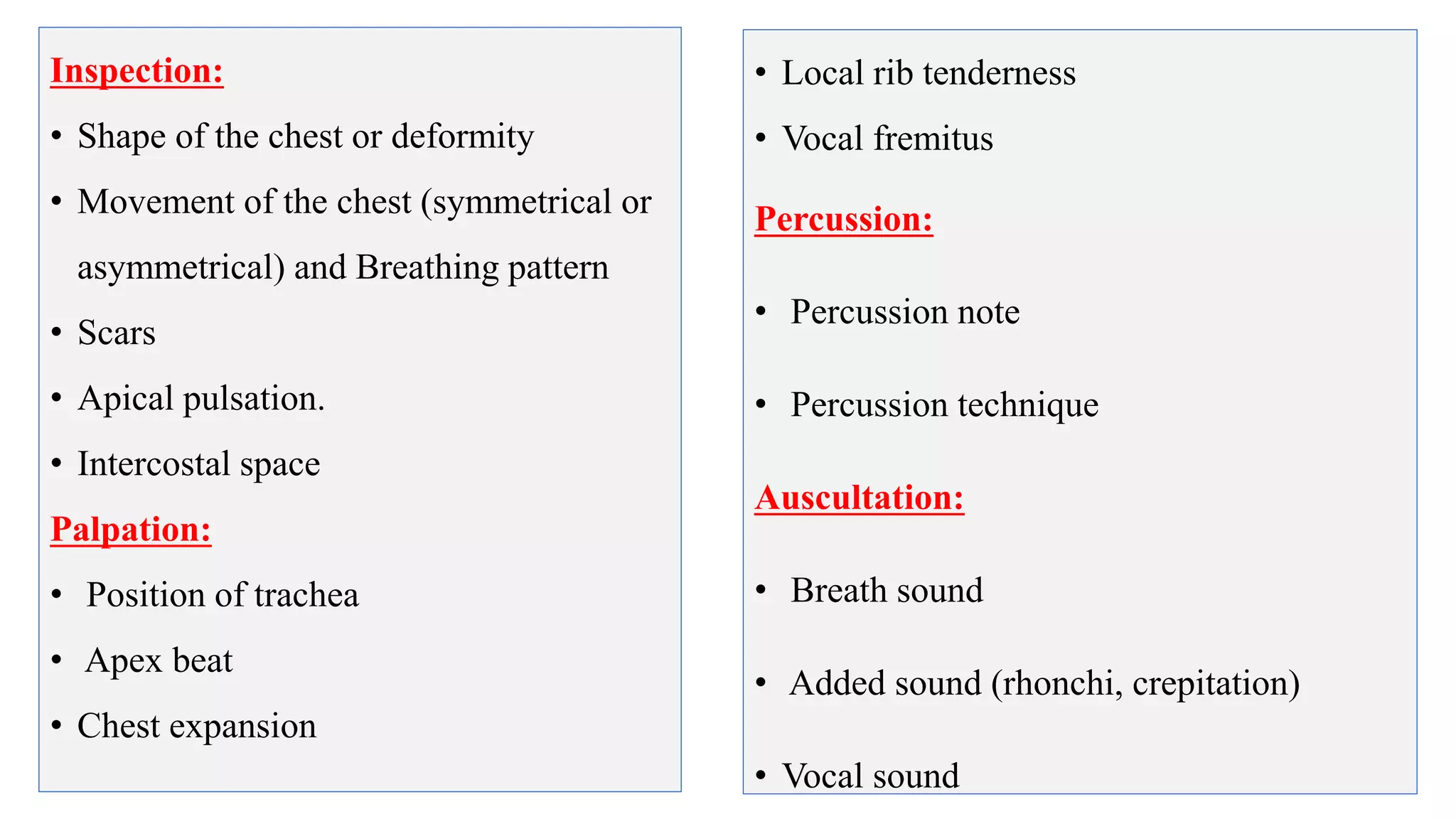
This document provides guidelines for performing a local chest examination, including inspection, palpation, percussion, and auscultation. The examination involves observing the patient's breathing patterns and chest shape, feeling the trachea, apex beat, and chest expansion, tapping to assess percussion notes, and listening for breath sounds, adventitious sounds like rhonchi or crackles, and vocal resonance. The examination is designed to evaluate the lungs, check for abnormalities, and compare both sides of the chest.